
Research Article | DOI: https://doi.org/10.58489/2836-497X/015
*Corresponding Author: Nihad Elsadig Babiker
Citation: Nedaa Ahmed Mohamed said, Nedaa Abd Alrahman, Sara Elsadig Babiker, Tyseer Alabid, Maye M. Merghani, Nihad Elsadig Babiker, (2023). Measurement of Methytetrahydrofolate Level among Sudanese Women with Hypertensive Disorders of Pregnancy, Khartoum state 2023, 2023. Archives of Gynaecology and Women Health.2(2). DOI: 10.58489/2836-497X/015
Copyright: © 2023 Nihad Elsadig Babiker, this is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 April 2023 | Accepted: 10 July 2023 | Published: 12 July 2023
Keywords: hypertensive pregnancy, pregnancy, hypertension, folate level, preeclampsia, gestational hypertension
Hypertensive disorders are a common complication of pregnancy that put women and their fetuses at disproportionate risk for further complications, as well as a life-long sequela. This study aimed to measure the Methytetrahydrofolate Level (folate) among Sudanese women with hypertensive disorders of pregnancy. This were a case-control hospital-based study conducted at the laboratory of the Omdurman maternity hospital – in Khartoum, Sudan during the period of January 2023 to March 2023. It included All patients attending Omdurman maternity hospital that diagnosed with hypertensive disorders of pregnancy, and apparently healthy women were included as a control group. ELIZA (mindary 8000) was used for folate level measurement. The mean of folate levels in the cases was (12.9± 3.7), and in the control group was (33.9±2.5), when compared the folate mean between the case and control group there was a highly significant decrease with (p. v= 0.001). While the folate level had insignificant differences with the history of hypertension and types of hypertensive pregnancy (p. v > 0.05). Also has appositive correlation with the age (p. v<0.05). In the Sudanese women with hypertensive pregnancy the folate level was significantly decreased when compared between the case and control group, and had insignificant differences with the history of hypertension, and types of hypertensive pregnancy and had a positive correlation with the age.
Hypertensive disorders of pregnancy are the most common medical disorders of pregnancy and are associated with increased maternal and prenatal risks, diagnosed on systolic blood pressure greater than or equal to 140 mm Hg and/or diastolic greater than or equal to 90 mm Hg [1]. Hypertension in pregnancy has 4 types: chronic hypertension, Preeclampsia, Gestational hypertension, and severe hypertension [2].
Methylenetetrahydrofolate reductase (MTHFR) plays a key role in folate metabolism by channeling one-carbon units between nucleotide synthesis and methylation reactions. Severe enzyme deficiency leads to hyper homocysteinemia and homocystinuria, with altered folate distribution and a phenotype that is characterized by damage to the nervous and vascular systems. Two frequent gene MTHF polymorphisms in humans confer moderate functional impairment of MTHFR activity for homozygous mutant individuals. The C to T change at nucleotide position 677, whose functional consequences are dependent on folate status, has been extensively studied for its clinical consequences. A second polymorphism, an A to C change at nucleotide position 1298, is not as well characterized [3].
Hypertensive disorders of pregnancy (HDP) are now considered to arise from a myriad of metabolic, immunologic, genetic, and environmental influences. The role of oxidative stress in the pathophysiology of PE has increasingly been postulated. The placenta continuously generates ROS, and the overproduction of ROS results in accelerated placental aging. Therefore, enzymatic mechanisms have naturally evolved to control or mitigate the effects of ROS through the generation of antioxidants such as glutathione (GSH), superoxide dismutase (SOD), and catalase (CAT) [4].
Available evidence similarly suggests that disorders of homocysteine metabolism may be involved in the pathophysiology of HDP. These metabolic processes are regulated by a complex array of enzymes and biochemical compounds including folate and vitamin B12 which function as substrates and cofactors. Methylenetetrahydrofolate reductase (MTHFR) is a rate-limiting enzyme in the remethylation of homocysteine. Methylenetetrahydrofolate reductase catalyzes the conversion of 5, 10-methylenetetrahydrofolate to 5-methyltetrahydrofolate, a co-substrate for homocysteine remethylation to methionine. In addition to dietary deficiencies of vitamins, mutations in the genes coding for enzymes involved in homocysteine metabolism may alter enzymatic levels or activities and may lead to elevated homocysteine concentrations. Accumulated homocysteine level is a risk factor associated with endothelial dysfunction, a key feature in the pathogenesis of HDP. Homocysteine is readily oxidized to homocysteine thiolactone resulting in the formation of free radicals and lipid peroxidation [4]. In Sudan, there aren’t clear published data related to this topic therefore this study was designed to measure the Methytetrahydrofolate level among Sudanese women with hypertensive disorders of pregnancy.
This was a case-control hospital-based study conducted at the laboratory of the Omdurman maternity hospital – in Khartoum, Sudan during the period of January 2023 to March 2023. It included All patients attending Omdurman maternity hospital that diagnosed with hypertensive disorders of pregnancy, and apparently healthy women were included as a control group. participants under folic acid therapy and those with a previous history of hypertensive disorders of pregnancy were excluded the study was approved by the ethical committee of a national university, faculty of medical laboratory, and the participants were fully informed about the advantages and disadvantages before participation in the research (verbal informed consent). From each participant, 3 ml of venous blood was collected in sterile plain containers. ELIZA was used for folate level measurement. SPSS version 23 statistical software (SPSS Inc., USA) was used for statistical analysis.
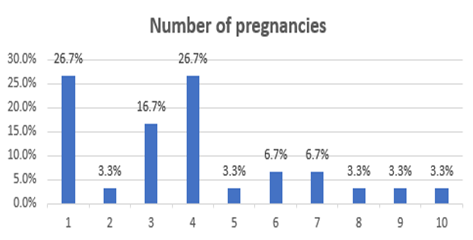
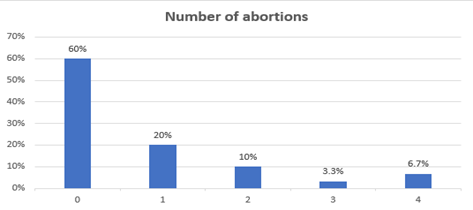
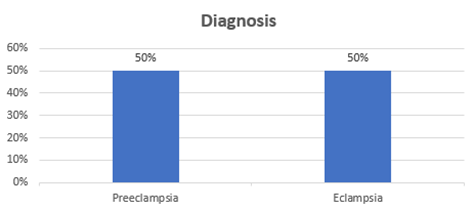
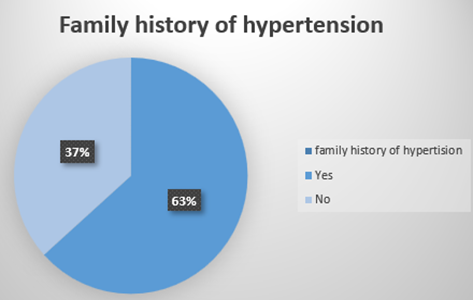
In the present study, a total of sixty participants were in roll, thirty as a case group and thirty as a control group. the mean age in the case group was (30.8±6.9) and in the control group was (28.9±5.5). in the case group, 20% had a history of abortion for one time, 26.7% had pregnancy for the first time, 50% were diagnosed as preeclampsia and50% were diagnosed with eclampsia, in addition, 63% had a family history of hypertension (table1) (figure 1, 2.3,4)
Table (1): Descriptive Statistics
| N | Minimum | Maximum | Mean | Std. Deviation | |
|---|---|---|---|---|---|
| Case | |||||
| Age | 30 | 18 | 43 | 30.8 | 6.9 |
| Control | |||||
| Age | 30 | 18 | 40 | 28.9 | 5.5 |
Hematological Result
In this study, the results revealed that; The mean folate levels in the cases were (12.9± 3.7), and in the control group were (33.9±2.5) (Figure 5). When comparing the folate mean between the case and control group there was a highly significant decrease with (p. v= 0.001) (table 2). While the folate level had insignificant differences with the history of hypertension and types of hypertensive pregnancy (p. v > 0.05). Also has a positive correlation with the age (p. v <0>
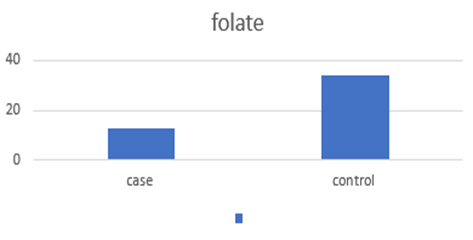
Table 2: Comparison of folate level between case and control
| Parameters | Study population | P. value | |
|---|---|---|---|
| Case (n=30) | Control (n=30) | ||
| Folate | 12.9 ± 3.7 | 33.9 ± 29.5 | 0.001* |
Table 3: Comparison of folate level according to the history of hypertension
| Parameters | History of Hypertension in the Family | P. value | |
|---|---|---|---|
| Yes (n=19) | No (n=11) | ||
| Folate | 37.2 ± 33.8 | 28.4 ± 20.3 | 0.439 |
Table 4: Comparison of folate according to the type of hypertensive pregnancy
| Parameters | Diagnosis | P. value | |
|---|---|---|---|
| Preeclampsia (n=15) | Eclampsia (n=15) | ||
| Folate | 28.7 ± 17.5 | 39.2 ± 9.8 | 0.338 |
Table 5: Correlations of age with folate
| Parameters | Age | |
|---|---|---|
| Folate | Pearson Correlation | .534 |
| P. value | .002* | |
Hypertensive disorders of pregnancy HDP are the second leading cause of global maternal mortality behind maternal hemorrhage and are a significant cause of short- and long-term maternal and fetal/offspring morbidity. Elevated systolic BPs throughout pregnancy, even below the diagnostic threshold for hypertension, also are associated with an increased risk of preterm delivery and infants who are small for gestational age and have low birth weight [5,6].
This was a case-control hospital-based study conducted at the laboratory of the Omdurman maternity hospital - Khartoum, Sudan during the period January 2023 to March 2023, and aimed to measure the Methytetrahydrofolate Level (folate) among Sudanese Women with Hypertensive Disorders of pregnancy the results revealed that; in the case group the mean of ages was (30.8±6.9), 20% had a history of abortion for one time, 26.7% had pregnancy for the first time, 50% diagnosed as preeclampsia and50% diagnosed as eclampsia, in addition, 63% had a family history of hypertension. This finding agreed with Liu X et al who reported; The risk of hypertensive disorders in pregnancy increases gradually with age in pregnant women aged over 35 years. And the risks of preeclampsia and eclampsia rise in teenage pregnancy. Better management helps to reduce the incidence of eclampsia and improve the outcomes of pregnancy in pregnant women with advanced maternal age and teenagers.Also, Sheen JJ et al said; With a changing demographic profile of preeclampsia, older women accounted for an increasing proportion of preeclampsia and related adverse outcomes [7,8]. Zhang et al mentioned; Preeclampsia and eclampsia carry a high risk for severe maternal morbidity. Compared to Caucasians, African Americans have a higher incidence of hypertensive disorders in pregnancy and suffer from more severe complications [9].
Previous studies have suggested that HDP is a primiparous disease, while a previous birth confers a protective effect on HDP, the protective effect may attribute to immune tolerance to paternal antigen in fetal cells, and also to improve trophoblastic invasion after modification of maternal spiral arteries during the previous pregnancy. However, whether induced abortion (IA), before which the woman has also been exposed to fetal cells, would offer similar protection against HDP in primiparous women is controversial. Some studies have shown that previous IA is protective against PE. At the other end of the spectrum, an IA in a first pregnancy was associated with a higher subsequent risk of PE [10].
Regarding the folate level in this study, the results revealed that; The mean folate levels in the cases was (12.9± 3.7), and in the control group was (33.9±2.5). When comparing the folate mean between the case and control group there was a highly significant decrease with (p. v= 0.001). While the folate level had insignificant differences with the history of hypertension and types of hypertensive pregnancy (p. v > 0.05). Also has a positive correlation with the age (p. v <0>
These results consist of Olapeju et al study which steady; Hypertensive disorders of pregnancy are a recognized risk factor for a woman's future cardiovascular risk. The potential role of micronutrients in mitigating hypertensive disorders is not fully understood. We found that pre-eclampsia disorders, but not gestational hypertension, were associated with lower folate and higher homocysteine levels postpartum, especially among black mothers. Also, Kharb et al said; Elevated homocysteine and folate and vitamin B12 deficiency during pregnancy may be a risk factor for preeclampsia and future risk of cardiovascular risk. Furthermore, Bibi et al study showed; Higher Homocysteine levels in pregnancies complicated by pre-eclampsia and eclampsia have been noted. Data support the hypothesis that folate, vitamin 812, and B6 lower hcy levels in hyperhomocysteinemia women [11,12,13].
Homocysteine (HCT) is a substance produced in the metabolism of methionine. It is an essential type of amino acid gained from the daily diet. Methylenetetrahydrofolate reductase (MTHFR) gene mutation is related to elevated total homocysteine (THCT) expressions, in particular, among women with low folate intake. Increased Hct in peripheral blood may lead to vascular illnesses, coronary artery dysfunction, atherosclerotic changes, and embolic diseases. Recent studies have reported that HCT was associated with numerous pregnancy complications, including recurrent pregnancy loss (RPL), preeclampsia (PE), preterm delivery, placental abruption, fetal growth restriction (FGR), and gestational diabetes mellitus (GDM). Besides, it was discovered that neonatal birth weight and maternal HCT levels were negatively correlated [14].
In addition, Yuan et al revealed; Lower SF levels were associated with higher risks of intrahepatic cholestasis of pregnancy, pre-eclampsia, and a lower risk of gestational diabetes mellitus. An imbalance between folate and vitamin B12, represented by a higher or lower SFVB12R before delivery, was significantly associated with adverse pregnancy outcomes [15].
Singh et al said; Dietary deficiencies of folate and other B vitamin cofactors involved in one-carbon metabolism, together with genetic polymorphisms in key folate-methionine metabolic pathway enzymes, are associated with increases in circulating plasma homocysteine, reduction in DNA methylation patterns, and genome instability events. All of these biomarkers have also been associated with pre-eclampsia [16].
another study reported; Placental infarction or abruption, recurrent pregnancy loss, and pre-eclampsia are thought to arise due to defects within the placental vascular bed. Deficiencies of vitamin B12 and folate or other abnormalities within the methionine-homocyst(e)ine pathway have been implicated in the development of such placental diseases [17].
Finally, the research results disagreed with
Serrano et al study which revealed that; Maternal serum concentrations of folate were associated as a protective factor for pre-eclampsia while concentrations of homocysteine were associated as a risk factor. No association between maternal vitamin B12 concentrations and preeclampsia was found [18].
In the Sudanese women with hypertensive pregnancy, the folate level was significantly decreased when compared between the case and control group, and had insignificant differences with the history of hypertension, types of hypertensive pregnancy, and had a positive correlation with the age.
There is a limitation regarding this study; there is a lack of data about the patient’s gestational ages, and the patient’s dietary intake, further research with a large sample size and clear data is needed.
The authors have no conflict of interest to declare.