Archive : Article / Volume 2, Issue 1
- Research Article | DOI:
- https://doi.org/10.58489/2836-502X/003
An update on the Genetics of Premature ovarian insufficiency (POI) with special emphasis on mini chromosome maintenance (MCM)8 &9-A Short Communication
- Scientific Director, Centre for Human Reproduction721, G.T.B. Nagar, Jalandhar-144001, Punjab, India
- Scientific Director, Ex-Rotunda-A Centre for Human Reproductio 672, Kalpak Garden,Perry Cross Road,Near Otterâs Club,Bandra(W)-400040MUMBAI,INDIA
- Consultant Neurologist, Swami Satyanand Hospital Near Nawi Kachehri, Baradri, Ladowali road, JALANDHAR, PUNJAB
Kulvinder Kochar Kaur
Kulvinder K.K., Gautam Nand K.A, Mandeep Singh, (2023). An update on the Genetics of Premature ovarian insufficiency (POI) with special emphasis on mini chromosome maintenance (MCM)8 &9-A Short Communication. Journal of Endocrine System and Diabetes. 1(1). DOI: 10.58489/2836-502X/003.
© 2023 Kulvinder K.K., this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- Received Date: 28-12-2022
- Accepted Date: 06-01-2023
- Published Date: 20-01-2023
POI; MCM8/9; HCC; CRC
Abstract
Objective- Premature ovarian insufficiency (POI) comprises of enhanced gonadotropins, specifically follicle stimulating hormone (FSH) and irregularity/ lack of menstruation inwomen< 40yrs of age.Having reviewed literatureearlier with a case report on genetics of POI with the advent of whole exon sequencing,here we aimed to update the same.
Methods-Relevant search engineswas done to update literature on genetics in POI emphasizing on the part of maintenance complex competence 8/9 (MCM8 and MCM9) in POIon what had not been covered earliertill date.
Results-On search it was evident that all the patients that manifested biallelic variations carrier of MCM9 presented with primary amenorrhea whereas the heterozygous carriers possessed greater probability of secondary amenorrhea. Further homozygous variations of MCM8,BRCA1 andRAD54L, were observed combined with MCM9 variations that coexisted in patients with MCM9 variations that coexisted in patients that pointed towards an accrual of action of genetic abnormalities impacted the robustness of POI. Furthermore, female mice with absence of Mcm8 or Mcm9 presented with infertility, which correlated with early germ cells elimination possessing a susceptibility for cancers,inclusive of Hepatocellular carcinoma (HCC)and ovarian tumors or hyperplasia. Recently in a Chinese cohort of 192POIwomen(192controls) 3 innovative heterozygous mutations were observed. Functional evaluation on HEK293 Kidney cells transfected with mutant plasmids illustrated that cells overexpressing mutant MCM9 possessed dysfunctional DNA repair ability besides haploinsufficiency of MCM9 was posited.
Conclusions-With homozygous mutation carriers of MCM9 presenting CRC, HCC emphasis is laid on long term follow up significance for tumor watching possibly by DNA replication correlated healing by sustenance of fork integrity at the time ofreplication stress.
Introduction
Premature ovarian insufficiency (POI) represents a heterogenous disorder, impacting 1/100women of reproductive age. By definition POI comprises of enhanced gonadotropins, specifically follicle stimulating hormone(FSH) along with irregularity or lack of menstruation prior to 40yrs of age. Considerable physical, mental besides economic load gets inserted on the patients with a diagnosis of POI besides resulting in disturbance of a woman’s reproductive capacity, however is correlated with an escalated risk of osteoporosis, cardiovascular disease as well as early mortality [1]. We had reviewed the literature on genetics of POI in 2016with a case report[2].In brief we detailed the genetics regarding POI with recent introduction of whole exon sequencing. Cytogenetic methods (array cGH) had identified other areas of interest but studies had not illustrated consistent outcomes , the resolution of array had differed and replicating it was uncommon .Whole exon sequencing in non-syndromic POI, had only begun recently as per 2016 where mutations in the stromal antigen 3 (STAG3), synaptonemal complex central element 3 (SYCE1), mini chromosome maintenance complex competence 8&9 (MCM8, MCM9) and ATP dependent DNA helicase homolog (HFMD gene)were observed .Hence Qin etal. [3],described together cytogenetic, cytogenetic (array cGH)and exon sequencing approaches had illustrated 20-25% of POI cases displayed a genetic etiology. Hence the remaining genes or causative genes would be promoted besides by whole genomic approaches which implicated long cohort in multiple populations along with further incorporated environmental exposure and exploring signaling pathways in intragenic and intergenicareas which point to disturbances incontrolling gene networks [3].
Akin to that Chapman et.al., [4], reviewed the genetic causes including oocyte specific transcription factors, like NR5A1, NOBOX like genes besides FIGLA and FOXL2 Genes and folliculogenesis growth factors like Bone morphogenetic protein15(BMP15) in addition Growth Differentiation factor9(GDF9) [of the TGFβsuperfamily growth factors] [4].
Further various micro-RNA’s like miR23a family facilitates granulosa cell apoptosis via supression of X linked inhibitor of apoptosis (XIAP) expression pointingto the differential expression of miR23a might be a potential candidate of POF generation. In view of small sample size, the role of mir23in the etiology of POF is unclear [5]. More currently Dang et al investigated differential expression miR in a large cohort of Chinese women and found 22 significantly up regulated and 29 down regulated miR in 140 POF patients, as compared to controls. Among these mir22-3pwas significantly down regulated in POF and a negative association between serum micro22-3pand FSH was observed.
The researchers pointed that miR22-3p may control pituitary FSH liberation, since its expression had been observed in the pig pituitary whereby the reduced expression had been observed toaid toward POF pathogenesis, Tsuilo, conducted a retrospective study on copy number variation analysis in 301 spontaneous POF patients with 3188 controls from 2003-2014 at Estonian Genome Centre at University of Tartu Biobankand found 11 novel microdeletions which encompass genes which were germane to POFeg [6]. FMN2 (Iq43) and SGOL (22q33.1) are essential for meiotic progression, while TBP (6q27), SCARB1 (12q24.31), BNC1 (15q25) and ARFGAP3 (22q13.2) were implicated in follicular growth along with oocyte maturation. They further validated the significance of recently invented hemizygous microdeletions of meiotic genes, SYCE1 (10q26.3) as well as CPEB (15q25.2) in POF patients. The limitations were no functional analysis was conducted [7].
Two main modes are implicated in POI namely i) follicular impairment as well as follicular elimination. Nevertheless, the etiology keeps eluding in maximum numbers of cases.The acknowledged etiology at present are constituted by i)medical/iatrogenic like ovarian surgery/cytotoxic cancer treatment,ii) medical as well as storage conditionsiii)infectionsiv) chromosomal aberrations as well as autoimmune diseases. Usually POI possesses a genetic background with over 50 genes,where mutations might constitute etiological factors besides involvement of numerous genes[8]. Besides total elimination of mutations, partial molecular aberrations might be causative in the unanticipated partial phenotypes. Genetic along with cytogenetic etiologic factors regarding nonsyndromic POI are implicated in 10-50% patients; chromosomal aberrations or occasional gene abnormalities have been detailed. Regarding non syndromic POI, of the autosomal genes, i) just occasional mutations of gonadotropin receptors or their ligands, ii)of growth factors[Bone morphogenetic protein15(BMP15) in addition Growth Differentiation factor9(GDF9)or iii)transcription factor(SF1), implicated in follicular generation, iv)of genes implicated in the follicular pool generation besides early enrolment[POF1B,FIGLA, NOBOX) as well as in near past regarding v)meiosis(cohesinlSTAG3) have been detailed. This robustly pointed towards extra genetic factors still required identification. These genes possess the capacity of impacting gonadal formation, replication of DNA/ meiosis along with DNA healing, hormonal signalling, immune function along with metabolism. An insight regarding ovarian physiology as well as biology aids in generating a scaffolding for interpretation of etiology of POI [8].
MCM8 along with MCM9, represent members of the minichromosome maintainance (MCM) family of genes (MCM 2- MCM 9) represent autosomal genes which have been detailed recently in resulting in Hypergonadotropic Hypogonadism on inheritance in an autosomal recessiveway in occasional consanguineous families. Female mice with absence of Mcm8 or Mcm9 present with infertility, correlated with early elimination of germ cells possessing a susceptibility for cancers,inclusive of Hepatocellular carcinoma(HCC) along with ovarian tumors or hyperplasia. in addition to that genome wide association studies(GWAS) regarding reproductive aging have isolated nonsense Single nucleotide polymorphisms (SNP) within the Mcm8 locushat illustrated the maximum robust correlation with age of menopause. These studiespointed that MCM8 along with MCM9 are necessary controllers of gonads right from their formation till senility. In view of this knowledge regarding central part of MCM8 along with MCM9 in reproductive aging the group of Rajkovic attempted assessment of MCM8 as well as MCM9 variants in a subset of subjects with POI .A study conducted recently has isolated considerable numbers of innovative probably variantsin MCM8 along with MCM9 in the recruited POI subjects[9] .
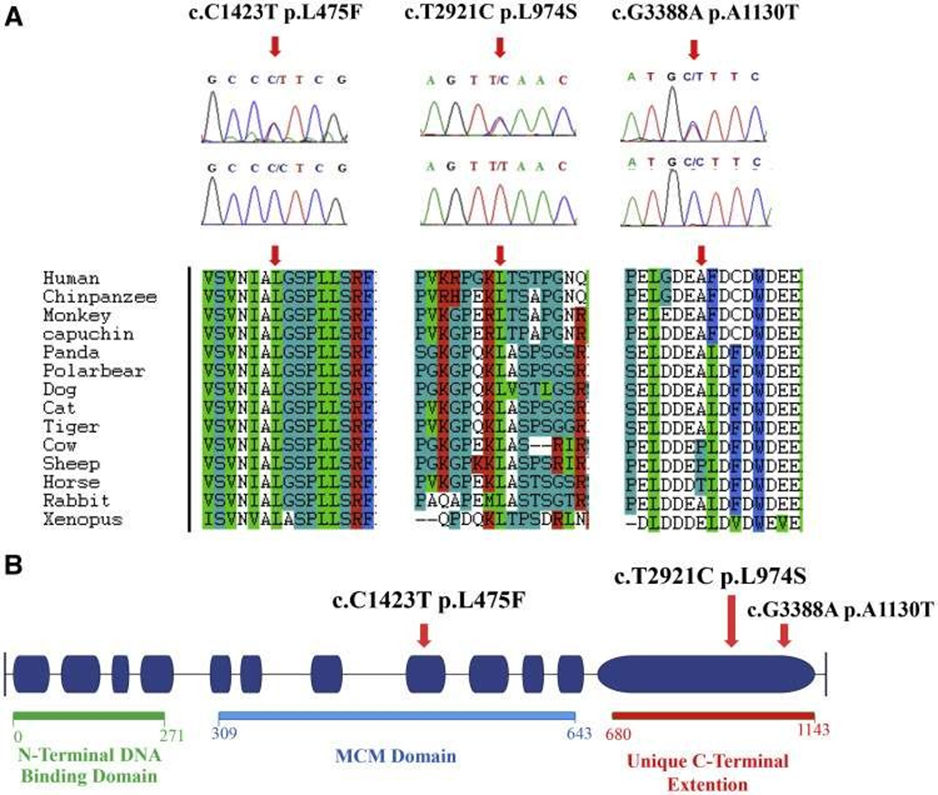
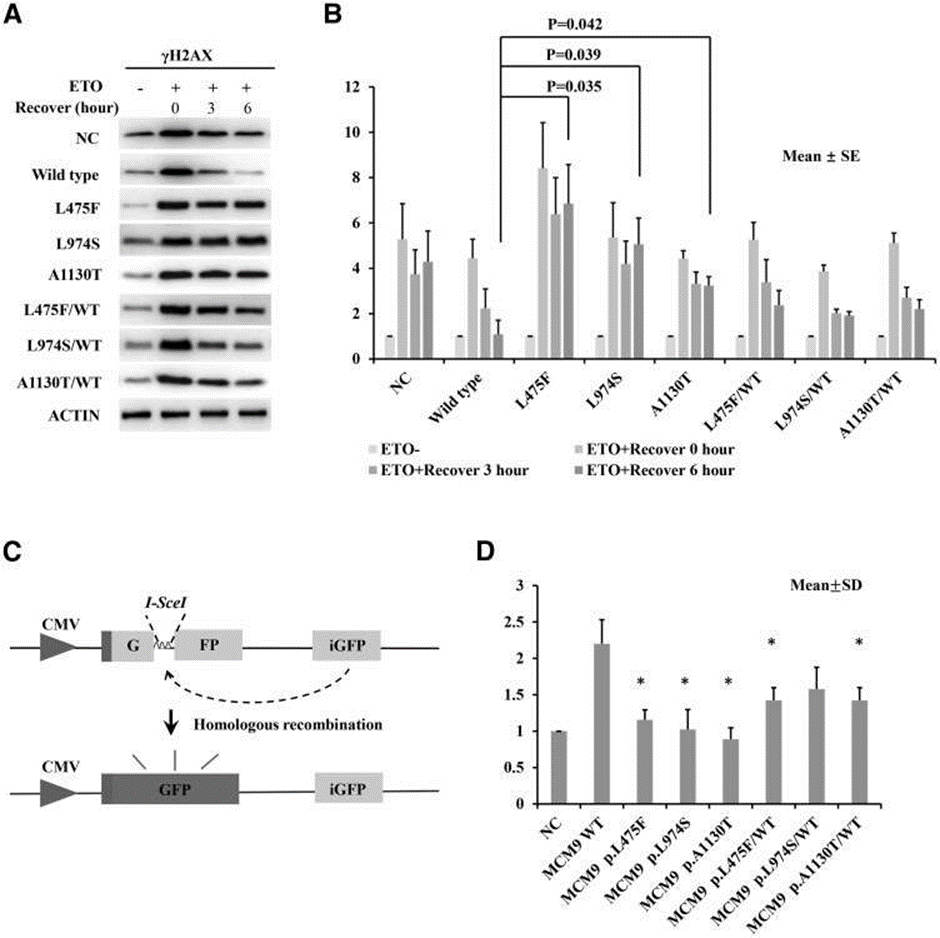
Guo etal.[10],detailed 3 innovative missense mutations of MCM9.Their objective was to find the properties of probable mutations amongst a Chines population comprising of patients with POI.192 cases with POI got recruited along with 192 controls. Sanger sequencing was conducted, where 3 innovative heterozygous mutations were isolated in 3 patients with POI. The same mutations were not observed in controls. Clinical phenotype of these 3 patients were practically similar to that of a normal puberty, along with manifestation in the form of secondary amenorrhea .On Pelvic ultrasonography it was illustrated that there were ovaries that were considerably small in size or were lacking .No follicle was visualized in each patient .For functional evaluation of the probable functional influence of these mutations(like a probable change of DNA healing) mutant plasmids were generated HEK293 Kidney cells from embryonic Kidney cell lines got transfected with mutant plasmids along with received treatment with etoposide for stimulating double strand breaks(DSB). DNA repair assays illustrated thatcells which overexpressed mutant MCM9 possessed dysfunctional DNA repair ability besides haploinsufficiency of MCM9 was posited (see figure1 &2).
Currently all the patients that manifested biallelic variations carrier of MCM9 possessed primary amenorrhea. Desai et.al., [9], observed that 1/151 patients possessed homozygous variations of MCM9, whereas 7 patients (7/151,4.6%) possessed heterozygous variations with a probable pathogenic action. Conversely ,the heterozygous carriers possessed greater probability of secondary amenorrhea that was in agreement with the phenotype seen in Qin’s cohort[10].Hence one can presumethat probability exists regarding the actions of MCM9 mutations on ovarian function might be dose based .Further Desai et.al., [9],further observed homozygous variations of MCM8,BRCA1 as well as RAD54L,in combination with MCM9 variations that coexisted in patients with MCM9 variations that coexisted in patients that pointed towards an accrual of action of genetic abnormalities impacted the robustness of POI.
Haploinsufficiency of MCM9 that resulted from heterozygous variations possessed a susceptibility for secondary amenorrhea, in view of residual functional MCM9,while biallelic variations might result in greater robustness in aberrant Ovarian generation(like primary amenorrhea).In case of their cohort, Yang et.al., [11], observed heterozygous variations in MCM8,BRCA1 as well as RAD54L, along with in combination with MCM9 variations that coexisted in patients that pointed towards an accrual of action of genetic abnormalities impacted the robustness of POI.
This particular study which validated the prior studies pointed to the significance of MCM8 along with MCM9 constituents regarding normal DNA replication which are key regarding gonadal formation as well as ovarian function. Future studies in addition to whole –exome sequencing would yield greater understanding regarding POI.
Conclusions
All these approaches despite their significance continue to be a research strategy, hence case to case discussion in the present of patient is required. As clinicians besides scientists we need to remember the significance of long term follow up it is imperative for the treating doctor managing long term replacement . Furthermore, it is necessary to do it in concert with those who are believed to be experts in this field, since insight regarding future fertility possibilities besides other ways for family generation requires to be detailed. For improvement of quality of life (QOL)of the woman it is incumbent to keep the woman updated to build her confidence. Lastly, regarding isolation of innovative gene variants it is to guarantee long term follow up to watch for as well as detail the generation of any new symptoms[12]. Furthermore, the association amongst MCM9in addition to tumors has persistent to be not clarified. The Mcm knockout mice possessed a greater risk of generation of HCC [13]. Goldberg etal. [14], documented a homozygous mutation carriers of MCM9 presented Colorectal carcinoma along with POI. Nevertheless, the3 mutation carriers of Guo etal’s cohort did not have any history of tumors. So, the emphasis on why long term follow up is so significant regarding watching for tumors, in particular the hormone sensitive tumors needs to be emphasized to the patients with MCM9 mutations. This might be in view of its role in DNA replication- correlated healing by sustenance of fork integrity at the time of replication stress[15].
References
- Bachelot A,Nicolas C,Bidet M,Dulon J,Leban M,Golmard R,etal. Long term outcomes of ovarian function in women with intermittent Premature ovarian insufficiency. Clin Endocrinol (Oxf) 2017; 86:223-8.
- Kulvinder Kochar Kaur,Allahbadia GN,Singh M. An Approach to a Patient of Amenorrhea - Case Report and Review of Literature on Premature Ovarian Failure (POF); Electronic Journal of Biology, 2016, Vol.12(4): 477-483.
- Qin Y, Jiao X, Simpson L, et al. (2015). Genetics of primary ovarian insufficiency: new developments and opportunities. Hum Reprod Update. 21: 787-808
- Chapman C, Cree L, Shelling AN. (2015). The genetics of premature ovarian failure: Current perspectives. Int J Womens Health. 7: 799-810.
- Yang X, Zhou Y, Peng S, et al. (2012). Differentially expressed plasma microRNAs in premature ovarian failure and the potential regulatory function in mir23a in granulose cell apoptosis. Soc Reprod Fertil. 144: 235-244.
- Dang Y, Zhao S, Qin Y, et al. (2015). microRNAs-22- 3pis downregulated in the plasma of Han Chinese patients with premature ovarian failure. Fertil Srteril. 103: 802-807.
- Tsuiko O, Noukas M, Zilina O, et al. (2016). Copy number variation analysis detects novel candidate genes involved in follicular growth and oocyte maturation in a cohort of premature ovarian failure cases. Hum Reprod. 31: 1913-1925.
- TuckerEJ,GroverSR, Bachelot A,Touraine P,Sinclair AH. Premature ovarian insufficiency:new perspectives on genetic causes and phenotypic spectrum. Endocrinol Rev2016; 37:609-25.
- Desai S,Wood-TrageserM,MaticJ,Chipkin J,Jiang H,Bachelot A,etal. of MCM8 and MCM9 nucleotide variants in women with Premature ovarian insufficiency. J Clin Endocrinol Metab 2017; 102:57-82.
- GuoT, ZhengY,Li G, Zhao S,Ma J,Qin Y.Novel pathogenic mutations in minichromosome maintainance components responsible for Premature ovarian insufficiency. Fertil Steril 2020;113(4):845-52.
- YangX, Touraine P,Desai S,Humphreys G,Jiang H,YatsenkoA, etal. Gene variants identified by whole –exome sequencing in 33 French women with Premature ovarian insufficiency.J Assist Reprod Genet 2019;36:39-45.
- Touraine P. Premature ovarian insufficiency: step-by step- genetics bring new insights. Fertil Steril 2020;113(4):767-8.
- LuoY,SchimentiC. MCM9 deficiency delays Primordial germ cell proliferation independent of ATMpathway. Genesis 2015; 53:678-84.
- Goldberg Y, HalpernN, Hubert A, Adler SN, Cohen S, Plesser-Duvdevani M, etal. Mutated CM 9 is associated with predisposition to hereditary mixed polyposis and Colorectal cancer. Cancer Genet 2015; 208:621-4.
- Griffin WC, McKenzy DR, Klinzing KN, Baratam R, Eliyapura A, Trakselis MA. A multifunctional role for MCM8/ MCM9 helicase complex in maintaining fork integrityduring replication stress. Nat Commun 2022; 13:5090.


