
Research Article | DOI: https://doi.org/10.58489/2836-3558/003
*Corresponding Author: Sefanur Kose
Citation: Sefanur Kose, Sumeyye Sekmen, Meltem Pusuroglu, Fatma Beyazal Celiker, Cicek Hocaoglu, (2022). Compare of Brain Anomalies and Psychopathology of Patients in a Psychiatric Clinic: A Retrospective Study. Psychiatry and Psychological Disorders. 2(1). 10.58489/2836-3558/003
Copyright: © 2022 Sefanur Kose, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 23 December 2022 | Accepted: 30 December 2022 | Published: 10 January 2023
Keywords: arachnoid cyst, cavum vergae, empty sella, mega cisterna magna
Background: In parallel with the development of neuroimaging methods, become increasingly possible to explore the relationship between mental disorders and structural brain lesions. It is aimed to examine the relationship between the clinicalfeatures and psychopathologies of psychiatric patients and their anomalies.
Methods: Two hundred-six female patients who were treated in Clinic of Psychiatry, Rize Training and Research Hospital between01/Jan/2016 and 31/Dec/2021 and had brain magnetic resonance imaging (MRI) were included in this study. Sociodemographic and clinical characteristics data form was recorded for each patient. Simultaneously, the size and location of the anomalies were recorded by scanning the brain MRI.
Results: When the brain MRI scans of the patients were evaluated, 56% of 206 patients had at least one of the related anomalies. Enlarged Virchow-Robin space (VRS) in 2.4%, mega cisterna magna (MCM) in 14.6%, total empty sella (ES) in 8.3%, partial ES in 27.7%, cavum vergae (CV) in 1.9%, hippocampal remnant cyst (HRC) in 17%and 6.8% had arachnoid cyst (AC) findings. When the sociodemographic data and clinical characteristics of the patients were compared with the brain MRI findings, a significant correlation was found between the presence of MCM and the use of antidepressant medication (p=0.026). A significant correlation was found between the presenceof AC, disease duration and regular treatment history (p=0.0002). No significant correlation was found between otherdata and MRI (p>0.05).
Conclusions: In our study, it is noteworthy that a higher rate of anomaly was detected in brain imaging of caseswith a history of psychiatric diagnosisand treatment comparedto the general population.
Psychiatry, which deals with emotions, thoughts and behaviors of humans, is a medical discipline that has maintained its mystery and importance from past to present. Unraveling the mystery of how the psychic apparatus works and elucidating the etiologies and pathogenesis of mental disorders have been one of the most importantmissions of psychiatry. Although the interest in the brain increased duringthe Egyptian periodbefore Christ, this interest continuedafter Christ with the work of scientists such as Galen and Ibn Sina. By examining the brain folds (gyrus), which region of thebrain works and how, the relationship betweenstructural and functional disorders in the brain and psychiatric diseases has been investigated since ancient times [1]. With Berger's definition of electroencephalography (EEG) imaging in 1929, non-invasive cerebral imaging methods also gained importance. With the introduction of computed tomography (CT) and magnetic resonance (MRI) imaging into practice, neuroimaging studies have become an important data source. Owing to functional magnetic resonanceimaging (fMRI) and positron emissiontomography (PET), which are widely used today, neuroradiology has reached a level that can overcome many problems for psychiatry [2]. The effect of neuroanatomical disorders on the develop-ment of mental disorders has been one of the main areas of interest of neuroimaging studies.Some of the brain anomalies that are thoughtto be associated with psychiatric disorders are, arachnoidcyst (AC) [3,4], empty sella (ES) [5], enlarged Virchow-Robin spaces (VRS) [6], hippocampal remnant cyst (HRC) [7], cavum vergae (CV) [8,9] and mega cisternamagna (MCM) [10- 12].
Arachnoid cyst (figure 1a) is a cavity locatedin the intra- arachnoid space, filled with cerebrospinal fluid (CSF), well delimited by peripheral structures and not connected to the ventricular system [13]. Most often they are located in the supratentorial area. It constitutes about 1% of all intracranial masses and is more common in men [14]. The exact mechanism of formation is still unknown, and they can often be developmental and lessoften acquired. It was thought to occur due to the division or diverticulum of the developing arachnoid. A newer concept for the arachnoid cyst of the middle fossais that the temporal embryonic meningesdo not merge when a Sylvian fissure is forming. Often in the arachnoid cyst is not accompanied by abnormalities of brain development. Acquiredly, they may develop secondary to neoplasms, infection, surgical intervention and hemorrhage of the brain. Most arachnoid cystsare smalland asymptomatic. About 5% of patients aresymptomatic, and symptoms are due to mass effect, which is usually the result of enlargement [15,16]. AC- related symptoms are usually related to the size and locationof the cyst, often causingheadache, nausea, dizziness, and convulsions [17]. Case reportssuggesting a possibleetiological relationship betweenarachnoid cyst and severe psychiatric symptoms and disorders have been reported[3,18,19]. The effects of the arachnoid cyst on cognition have been extensively researched and have been shown to impair executive functions as well [4]. It was observed that anxiety and depression scores,which were higher in AC cases comparedto the normal population, normalized after surgical cyst decompression [17]. In the treatment of arachnoid cysts, some clinicians recommend surgery for symptomatic cases, while another group of clinicians recommends surgeryfor asymptomatic cysts in terms of possible complications. The most effective surgical treatments are excision of the external membrane of thecyst and cystoperitoneal shunt [20].
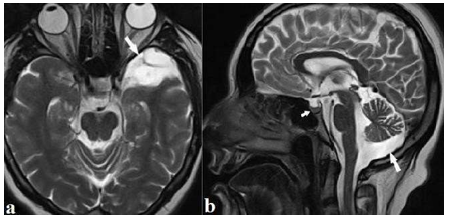
Mega cisterna magna (figure 1b) is the cisterna magna, which provides the transfer of cerebrospinal fluid (CSF) from the fourth ventricle to the foramen Magendi, is wider than 10 mm with the development of a posterior membrane defect during embryogenesis. This developmental variation in the posterior fossa does not morphologically affect the vermis and cerebellar hemispheres [21]. Approximately 1% of newborns have MCM. It constitutes 54% of all cystic posterior fossa malformations [22]. Although known that it is an incidental finding in neuroimaging and does not requirefollow-up, there are studies emphasizing that this anomaly may be associated with psychiatric disorders [10-12,23].
Empty sella (figure 1b) is a radiological finding in whichthe sella turcica is partial(less than 50%) or total (more than 50%) filled with CSF and the pituitary gland is flattened. It may developprimarily due to increased intracranial pressure or CSF passage throughthe diaphragmatic cella and secondarydue to loss of pituitaryvolume. It is more commonin female and obese patients. Although it is known to be an asymptomatic finding in general, hormonal irregularity was observed in 52% of the meta-analyses[24]. The symptoms of empty sella syndrome (ESS) are headache,visual disturbances and hormonal dysfunction [25]. ESS can also manifest itself with a variety of neuropsychiatric symptoms secondary to endocrine abnormalities or electrolyte imbalance. Although there are psychiatric casesin the literature that show a relationship withempty sella, the relationship betweenempty sella and psychiatric disorders has still not been proven[5,26,27].
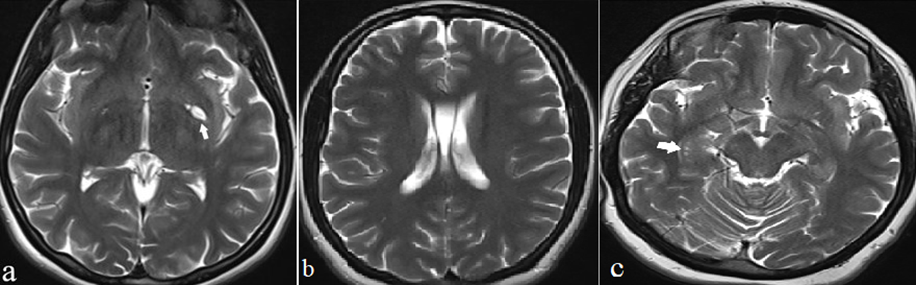
An enlarged VRS (figure 2a) is an expansion of the interstitial fluid filled VRS that surrounds the capillaries on the brain parenchyma. These gaps, which are normally1-2 mm wide, can be seen at any age, but they become more visible radiologically with increasing age. Although there is no consensus on the definition of the enlargement of the VRM, two milimeters has been accepted as the limit in some studies[28]. Previously, enlarged perivascular spaces were considered as artifact of histopathological fixationor were thought to be caused by loss of brain tissueduring aging. However, in the last 10 years, it has been observed that they can cause common neuropsychiatric findings [29,30]. Neuropsychiatric diseases such as depression, dementiaand psychosis accompanied by enlarged VRS are found in the literature [6]. The septum pellucidum is a thin layer with two laminas that forms the medial wall of the lateral ventricles. In normal fetal development, these two laminae unite to form the posterior half of the septum at about six months, while the anterior fusion is completed between the third and sixth monthsafterbirth. The gap formed between the two laminae as a result of not being fused is called the cavum septum pellucidum (CSP). CSPs smallerthan 6 mm are considered anatomical variants [31]. Cavum vergae (figure 2b) is the result of no fusion of SP and is the mostsevere form of CSP. CSP often accompanies CV. Isolated CV is extremely rare. CV and CSP may be present as an asymptomatic variation in some individuals. However, several epidemiological studies have suggestedthat their long-termpresence in the brain may lead to developmental abnormalities in midline structures, the limbic system of the brain, and various neuropsychiatric disorders [32]. Studies have been conducted on the relationship with many psychiatric disorders such as schizophrenia and bipolaraffective disorder(BAD) (8, 9). Hippocampal remnant cyst (figure 2c) is a change in signal intensityin a small area, usuallyin the hippocampus, on MR images. Typically, round or curvilinear, they are 1-2 mm in diameter. They are thoughtto be remnants of inadequateinvolution of the embryonic hippocampal fissure. It is usually localizedlaterally, at the apex of the hippocampal fold, between the Ammon’s horn and the dentate gyrus. Specific clinicalsigns or symptomsdo not accompany this anomaly [33-35]. Although some studies have reported that this variation is greater in Alzheimer's patients, no study has been found regarding its relationship with psychiatric pathologies [7].
In our study, we examined the frequency of anomalies observed by scanning the brain MRI images of patientswho were treated as inpatients in our service within the last 5 years, the location and size of the anomalies, sociodemographic data and psychopathology relationship. Although there are case reports associated with these anomalies in the literature, we could not reach a large-scale study in which many anomalies were screened together. Therefore, our studywill contribute to the current literature.
The study is a retrospective study conducted at the Department of Psychiatry, Rize Training and Research Hospital. Patientswho were admittedto the clinic between 01/Jan/2016-31/Dec/2021 were included in this study. Betweenthese dates, a total of 504 female patients were followed up and treatedin the clinic. In the hospital information system scan, 229 cases with brainMR imaging were reached. Twenty-three patients were not included in this study due to lack of data. Sociodemographic and clinical characteristics were recorded for each of the 206 patients. By examining the brain MRI scans, arachnoid cyst, empty sella, enlarged Virchow-Robin spaces,hippocampal remnant cyst,cavum vergae, mega cisterna magna anomalies were scanned, and the size and location features of these anomalieswere noted.
The protocol of this study was approved by the Recep Tayyip ErdoğanUniversity Non-Invasive ClinicalResearch Ethics Committee (10/Mar/2022-2022/66, E- 64247179-799). Written informed consentform was obtained from all patients participating in this study, and the Declaration of Helsinki was adhered to throughout this study.
Sociodemographic and clinical characteristics: in addition to sociodemographic data such as age, gender,marital status, educational status, occupation, accompanying medical disease, cigarette-alcohol- substance use, family history, psychopathological diagnoses according to DSM-5, durationof disease, number of hospitalizations and duration and medications were questioned. In addition, neuroimaging features (type, size and location) were recorded.
Brain MR images were obtained with 1.5 T device (SiemensMagnetom Aera, Erlangen,Germany). Imaging protocol is T1-weighted in the axial plane (TR 417 ms, TE 8,9 ms, slice thickness 5 mm), T2-weighted in the axial plane (TR 5480 ms, TE 100 ms, slice thickness 5 mm), T2-weighted in the sagittal plane (TR5480 ms, TE 100 ms, slice thickness 5 mm) and T2 FLAIR (TR 6000 ms, TE 86 ms, slice thickness 5 mm) images were used.
The data of this study were used with SPSS for Windows
25.0. Mean and standard deviation values, median and quartiles were used as descriptive statistics. Numbersand percentages were given for categorical variables. Compliance with the normal distribution was checked with the Shapiro-Wilk test. Data that did not show normaldistribution were compared between two independent groups using the Mann Whitney U test. If the number of Table 1. Brain MRI Findings of the Patients groups was more than two, the Kruskal-Walli’s test was used. Chi-square test was used to compare categorical data. For all comparisons, p < 0>
Since our study was conducted in the women'sclinic, the sample was made of female patients. The mean ageof the patients was 42.6 ± 14.2 years (17-81 years). Of the patients, 28(13.5%)had never been to school,100 (48.3%) were primary school graduates, 23(11.1%)were secondary school graduates, 38(18.4%) were high school graduates, 17(8.2%)were university graduates. 123(59.4%) were married,64(30.9%) were single, 11
(5.3%) widows, 8(3.9%) divorced.
Of the patients, 52(25.2%) had depressive disorder, 16 (7.8%) had anxiety disorder, 52(25.2%) had schizophrenia and related disorders,50(24.3%) had bipolaraffective disorder, 9(4.4%) had obsessivecompulsive disorder and 13(6.3%) were followed up with the diagnosis of dissociative disorder.
Brain MR imagingof the patients was evaluated.Of the
206 patients,56% had at least one of the related anomalies. Enlarged VRS in 2.4%, MCM in 14.6%, total ES in 8.3%, partial ES in 27.7%, CV in 1.9%, HRC in 17%, and AC in 6.8% of the patients(Table 1).
| N | % |
Enlarged Virchow Robin Space |
|
|
Yes | 5 | 2,4 |
No | 201 | 97,6 |
Arachnoid Cyst |
|
|
Yes | 14 | 6,8 |
No | 192 | 93,2 |
Arachnoid Cyst Diameter |
|
|
<1> | 4 | 1,9 |
1-2 Cm | 5 | 2,4 |
2-3 Cm | 3 | 1,5 |
> 3 Cm | 2 | 1 |
Mega Cisterna Magna |
|
|
Yes | 30 | 14,6 |
No | 176 | 85,4 |
Total Empty Sella |
|
|
Yes | 17 | 8,3 |
No | 189 | 91,7 |
Partial Empty Sella |
|
|
Yes | 57 | 27,7 |
No | 149 | 72,3 |
Cavum Vergae |
|
|
Yes | 4 | 1,9 |
No | 202 | 98,1 |
Hippocampal Remnant Cyst |
|
|
Yes | 35 | 17 |
No | 171 | 83 |
A significant relationship was foundbetween MSM and drugs (p=0.026). A significant correlation was found between the presence of AC and the historyof regular treatment(p=0.0002). There was no significant relationship between otherdata and MR imaging (p>0.05) (Table 2).
Table 2. Relation of Clinical Characteristics of Patients and MR Findings
| Age | Psychopathology | Regular treatment history | Medıcal Disease | |
P | ||||
| Enlarged VRS | 0.93 | 0.518 | 0.888 | 0.646 |
| Arachnoid Cyst | 0.69 | 0.311 | 0.0002 | 0.97 |
| Mega Cisterna Magna | 0.929 | 0.924 | 0.797 | 0.17 |
| Partial Empty Sella | 0.164 | 0.87 | 0.371 | 0.081 |
| Total Empty Sella | 0.029 | 0.263 | 0.521 | 0.763 |
| Cavum Vergae | 0.13 | 0.559 | 0.647 | 0.678 |
Hippocampal Remnant Cyst |
0.101 |
0.236 |
0.478 |
0.92 |
Chi-Square Test,
Mann Whitney U Test, P<0>
Of the patients with mega cisterna magna (MCM), 10 were using antidepressants, 7 were using antipsychotics, 6 were using antidepressants and antipsychotics, 6 were using antipsychotics and mood stabilizers, and one was using antidepressants, antipsychotics and mood stabilizers.
While 10 patients with a history of regular treatment had arachnoid cysts, 3 patients without regular treatment had arachnoid cysts (Table 3). Information on the coexistence rates of brain anomalies and psychopathologies can be found inTable 4.
Table 3. Frequency of Mega Cisternaand Arachnoid Cyst
| MCM | AC | |||
| N | N | |||
Drugs | Regular treatment history | |||
| Mood Stabilizers | 0 | 10 | ||
| AD | 10 | 3 | ||
| AP | 7 | |||
| AD, AP | 6 | |||
| AD, Mood Stabilizers | 0 | |||
| AP, Mood Stabilizers | 6 | |||
| AD, AP, MoodStabilizers | 1 | |||
| Total | 30 | |||
| AD: Antidepressants, AP: Antipsychotics | ||||
Table 4. Comparison of neuroimaging findingsand psychopathologies
Neuroimaging Finding | |||||||
Enlarged VRS |
AC |
MCM |
Partial ES |
Total ES | Cavum Vergae |
HRC | |
| n(%) | n(%) | n(%) | n(%) | n(%) | n(%) | n(%) | |
| DD | 2(0.9%) | 2(0.9%) | 8(3.8%) | 16(7.7%) | 5(2.4%) | 0(0%) | 11(5.3%) |
| AD | 0(0%) | 2(0.9%) | 2(0.9%) | 3(1.4%) | 2(0.9%) | 0(0%) | 5(2.4%) |
| SCH-SAD | 1(0.4%) | 6(2.9%) | 7(3.3%) | 14(6.7%) | 5(2.4%) | 1(0.4%) | 8(3.8%) |
| BAD | 0(0%) | 1(0.4%) | 7(3.3%) | 16(7.7%) | 2(0.9%) | 2(0.9%) | 3(1.4%) |
| OCD | 0(0%) | 0(0%) | 2(0.9%) | 2(0.9%) | 0(0%) | 0(0%) | 2(0.9%) |
| DIS. D. | 1(0.4%) | 1(0.4%) | 3(1.4%) | 2(0.9%) | 3(1.4%) | 0(0%) | 3(1.4%) |
| OTHER | 1(0.4%) | 2(0.9%) | 1(0.4%) | 4(1.9%) | 0(0%) | 1(0.4%) | 3(1.4%) |
| DD: Depressive Disorder, AD: Anxıety Disorder, SCH: Schızophrenıa, SAB: Schizoaffective Disorder BAD: Bipolar Affective Disorder, OCD: Obsesive compulsive disorder, DIS. D: Dissociative Disorder | |||||||
The relationship between the frequency, location and size of brain anomalies of the patients followed in our clinic for a 5-year period with their sociodemographic data and psychopathology was investigated. In our study, the prevalence of arachnoid cyst, mega cisterna magna, partial/complete empty sella, CV anomalies was found to be high compared to the general population. The frequency of enlarged VRS and HRC was similar to previous population studies. A significant relationship was found between MSM and medications and between AC and regular treatment history, and these data were evaluated randomly.
When the sociodemographic data of the patients were compared with a current study conducted in Ankara, they reached similar results in terms of average age and marital status. In our study, 61,8% of the patients graduated from primary school at most, and this rate is quite high compared to other studies [36]. It was thought that the low level of education could be due to the fact that it was made in a small center and that our patient group consisted of only women. It was thought that the high rate of 88,9% of our patients not working was due to female gender and mental illnesses.
When the diagnoses of our patients are compared with other studies, the rate of patients with depressive disorder is similar, but the diagnosis of schizophrenia and related disorders is lower at a rate of 25,2% compared to similar studies.The rate of bipolar affective disorder, which is 24.3%, is higher (36). Considering that psychotic disorders are observed more frequently in the male population and mood disorders are observed more frequently in the female population, we think that this rate difference is due to the inclusion of only female patients in our study.
The prevalence of arachnoid cysts was 6.8% in our patients and was significantly higher than the rate of 1.4% in a large-scale study. Although it is known that arachnoid cysts are significantly higher in males, we think that the higher incidence of AC in our study, which consisted of only female patients with a small population, was due to a sample consisting of psychiatric patients(15). As a result of the comparison of the presence of arachnoid cyst with sociodemographic and clinical features, a significant relationship was found only between the presence of regular treatment history (p=0.0002). It is very difficult to prove whether arachnoid cysts have an effect on psychiatric symptoms. But given the anatomical changes, we cannot exclude the possibility that the lesion has an important role in the occurrence of psychiatric symptoms. In our study, 42.8% of the cases with arachnoid cyst had a diagnosis under the heading of psychotic disorder. mIt has been suggested in some studies that arachnoid cysts may be responsible for psychosis-like conditions. Khandanpour et al found incidental cerebral lesions including arachnoid cysts on MRI in 62.5% of psychosis patients [37,38]. In our study, 11.5% of psychosis patients had AC. In 50% of the psychosis cases with arachnoid cyst in our study, the lesion is located in the anterior part of the left temporal lobe. Although this finding may be coincidental, we think that it may be a significant finding based on studies supporting the relationship between the left temporal lobe and psychosis [39].
In our study, mega cisterna magna anomaly was detected in 14.6% of the patients and the prevalence was quite high compared to 1% of a large-scale prevalence study. Among the scanned data, a significant relationship was found between MCM and medications used (p=0.026). Although it is known that MCM does not structurally affect the cerebellum, there are case reports suggesting that it may have affected functionally [12,13]. Because the cerebellum, which is typically known for its motor function, has connections with the emotional processing areas of the brain, shown in studies that cerebellar dysfunction is accompanied by cognitive and affective symptoms. In our study, determined that 50% of the patients with MCM lesions were diagnosed with mood disorders such as BAD and depressive disorder. Although this finding is not evidence of the relationship between mood regulation and the cerebellum, thought to be a remarkable finding.
Although the prevalence of primary empty sella is not fully known, reported that its prevalence varies between 2% and 20% [24,40]. In one study, empty sella was found in 1.94% of patients in the retrospective examination of brain MRI scans of a total of 12,414 patients [41]. In patients hospitalized in the psychiatric clinic, partial empty sella was detected in 27.7% of patients and total empty sella was detected in 8.3% of patients. The fact that we detected a higher rate of ES in psychiatric patients than in the general population in our study may be incidental. It can also be considered as data that can support the argument that empty sella may be associated with psychopathologies. Although the causal relationship between hypopituitarism and psychosis is not clear, known that psychosis can arise directly from a hormonal deficiency [42]. In our study, 36.5% of psychotic cases had empty sella; 25.6% of the cases with empty sella had psychosis and 52.7% had mood disorders such as depressive disorder or BAD. Although these findings are not evidence, they contribute to the importance of endocrinological pathologies in the etiopathogenesis of psychiatric disorders.
The enlarged VRS prevalence is not clear due to the different threshold values used for identification. However, in a retrospective study of 816 people in the literature, where the threshold value for the definitionof enlargement wasaccepted as 2 mm, the prevalence was determined as 6.3% [43]. In our study,enlarged VRS was detected in 2.4% of psychiatric patients.In a large meta-analysis study, an enlarged VRS was associated with lacunar microhemorrhages due to aging, hypertension, and small vessel disease [44]. In our study, there were very few cases with enlarged VRS,and when the relationship with other data was investigated, a statistically significant result could not be reached.
The incidence of CSP was found to be1%-85% in healthy adults [31]. Since the section thickness of the MR imaging used in our study was high,only CV was scanned instead of CSP. Clear data on the frequency of CV couldnot be found in the literature and cavum vergae was detected in 1.9% of the patients. It has been thought that CSP and CV may also indicate developmental anomalies in midlinestructures and that limbic system dysgenesis is one of the important underlying causes of psychiatric diseases [45]. In aretrospective study conducted with112 BAD and 87 schizophrenia patients in a study conducted in our country, 78.1% of patients in theschizophrenia group and 50.9% of patients in the BAD group had CSP. In schizophrenia, the prevalence of CSP increased compared to BAD and itsdimensions were larger. The rate of CSPwashigher in bipolar disorder with psychotic findingsthan inbipolar disorder without psychotic findings [9]. In our study, CV was detected in 4% of the patients with bipolar disorder and in 1.9%of psychosis patients.Since there are no prevalence studies on cavum vergae,theserates could not be compared. However, the fact that the patients with CV found to have 50
The authors have no financial interest to disclose
Acknowledgment
This study generally did not receive any grant and/or financial support from any institution and/or organization. We would like to thank all the healthcare workers who sacrificed during the pandemic.