Current Issue : Article / Volume 3, Issue 1
- CLINICAL AND MEDICAL IMAGES | DOI:
- https://doi.org/10.58489/2836-8630/010
Congenital Anonychia: Cooks Syndrome Variant or New Disease?
1,2Universidad Privada Del Valle, Facultad de Medicina, Cochabamba, Bolivia.
Camila F. Villarroel-Maldonado*
Camila F. Villarroel-Maldonado, Carlos G Teran., (2024). Congenital Anonychia: Cooks Syndrome Variant or New Disease? Journal of Clinical Pediatrics and Care. 3(1); DOI: 10.58489/2836-8630/010
© 2024 Camila F. Villarroel-Maldonado, this is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- Received Date: 05-03-2024
- Accepted Date: 18-04-2024
- Published Date: 09-05-2024
Abstract
Cooks syndrome, which was first reported by Cooks et al in 1985 is characterized by family history of bilateral congenital nail hypoplasia of digits 1,2 and 3, with absence of nails in digits 4, 5, and brachydactyly of the fifth finger of the hands and complete absence of toenails. In addition, there is hypoplasia or absence of distal phalanges of the hands and feet. According to the Office of rare Diseases of the National Institutes of Health, this syndrome is considered as a ârare diseaseâ. We present an 18 month old infant with history of congenital anonychia in digit 2 in both hands and feet and nail hypoplasia in digits 1 and 3 sparing digits 4 and 5. X-ray showed no abnormalities in phalanges, which is possibly a variant of Cooks Syndrome or a new disease with a strong family history of similar deformities involving the mother, grandmother, and sister.
Introduction
Cooks syndrome is an extremely rare condition with unknown prevalence, and even rarer a phenotypic variation. Congenital hereditary nail conditions are much more exceptional than those acquired because there are several genes involved in nail development during embryonic time. In 1985, Cooks described a “rare disease” in seven members of a family, characterized by a particular form of nail dysplasia with bone abnormalities. Their hands presented Progressive hypoplasia of the nails on digits 1-3, absence of 4-5 nails and brachydactyly of the thumbs. With the complete absence of all toenails and hypoplasia of each distal phalange. [1]
The exact etiology of this syndrome is still unknown, but according to Cooks, the probable mode of transmission is autosomal dominant.
Microduplications on chromosome 17q24.3 and involvement of a non-coding element of the SOX9 gene (17q24.3) have been associated with Cooks syndrome in four patients. The S0X9 gene is necessary for chondrocyte differentiation and cartilage formation [2].
Background
We present a novel case corresponding to a male infant, 18 months of age. Physical examination was normal, except for the appearance of his hands and feet. The findings included complete absence of nails in digits 2 and hypoplasia of nails in digits 1 and 3 with nails on digits 4 and 5 spared. The pattern was similar in hands and feet. [Fig 1 panel A, B] Radiography revealed no skeletal anomaly [Fig 1 panel D]. Mother had similar findings [Fig 1 Panel C].
In addition to this, the mother, recalled the family history of congenital hypoplasia/anonychia, similarly affected, with 2 of her 4 kids involved. The patient’s father was found to have normal nails in hands and feet. Among the affected members were his grandmother, mother, and sister. His mother had 3 sisters, and none of them present anomalies. She had 4 kids: The first one was not affected, the second was affected, the third one was normal, and the 4th one which is our patient; affected. All of those presenting the abnormality had the same level of the severity and daily life activities are not compromised in any way by this condition.
Discussion
Anonychia, or absence of nails, is rare. It may be congenital or acquired due to trauma in the nail matrix, medications including anticonvulsants and warfarin, or in a variety of genetic syndromes; as Nail Patella, Fryns, Turner, among others. (3)
Anonychia or nail Hypoplasia, with phalangeal hypoplasia, may occur as a part of multiple congenital syndromes. Most of these syndromes are autosomal dominant disorders. Cooks proposed this inheritance pattern of absence/hypoplasia of nails and distal phalanx, at birth and often bilateral, affecting hands and feet, describing seven individuals in two generations, with one instance of male-to-male transmission with probable autosomal dominant transmission. (4)
In the presented case, we would like to propose the possibility of an X linked dominance by mutation in the x chromosome [Figure 2]. In females, a mutation in one of the two X chromosomes would be enough to cause an abnormality; in males, the only copy of X could be the cause of this condition. X linked disorders are seen more commonly in females than males. Fathers cannot pass x linked to their sons, but all daughters of affected fathers will be affected and can pass it to their children.
Affected females can transmit the mutant allele to 50% of their male offspring and 50% of their female offspring. [5]
The main findings in our case and his family may represent either a Cooks syndrome variant, without the radiological features of hypoplasia/absence of distal phalanx or a different pattern of disease not described before. In addition, we would like to refute the male-to-male transmission proposed by Cooks, considering our case, where we found female to female transmission that strongly points to an X linked autosomal dominant inheritance pattern [Figure 2].
Unfortunately, genetic studies were not performed on our patient, and presumptions of Cooks syndrome diagnosis was established based on the clinical observations. In certain conditions as the one reported, specialized genetic testing may be required to understand this rare disease further, unfortunately the lack of medical and economical resources becomes a strong limitation in the presence of rare genetic disorders, like this one.
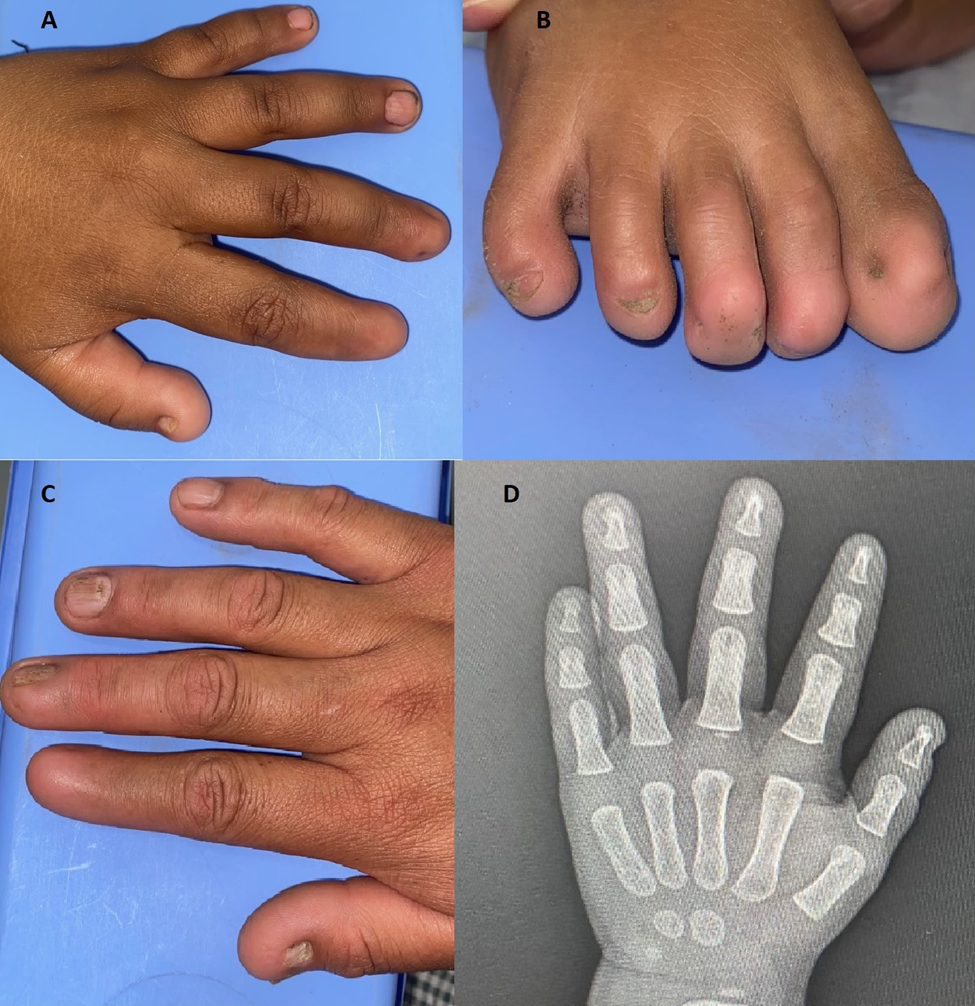
Fig 1: complete absence of nails in digits 2 and hypoplasia of nails in digits 1 and 3 [panel A, B]. Mother’s hand shows similar findings [Panel C]. Radiography revealing no skeletal anomalies [panel D].
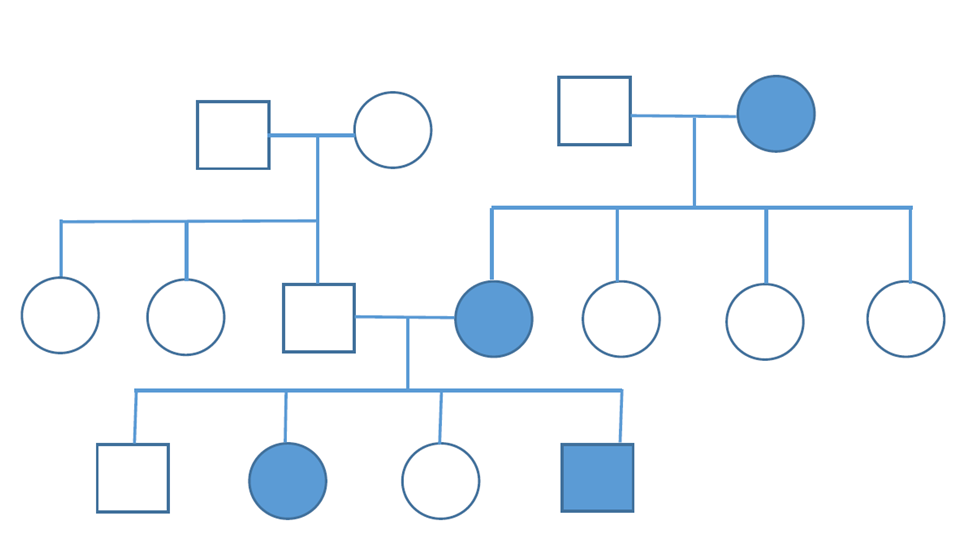
Fig 2: female to female transmission indicating an X linked autosomal dominant inheritance pattern
Ethical committee and consent
Informed consent from parents was approved and an ethical committee from the hospital approved the case and manuscript.
Conflicts of interest
The authors declare no conflicts of interest.
References
- Cooks, R. G., Hertz, M., Katznelson, M. B. M., & Goodman, R. M. (1985). A new nail dysplasia syndrome with onychonychia and absence and/or hypoplasia of distal phalanges. Clinical genetics, 27(1), 85-91.
- Kurth, I., Klopocki, E., Stricker, S., van Oosterwijk, J., Vanek, S., Altmann, J., ... & Mundlos, S. (2009). Duplications of noncoding elements 5′ of SOX9 are associated with brachydactyly-anonychia. Nature genetics, 41(8), 862-863.
- Seitz, C. S., & Hamm, H. (2005). Congenital brachydactyly and nail hypoplasia: clue to bone‐dependent nail formation. British Journal of Dermatology, 152(6), 1339-1342.
- Brennan, C. B., Buehler, T., & Lesher Jr, J. L. (2013). Cooks syndrome: A case report and brief review. Pediatric dermatology, 30(4), e52-e53.
- Basta M, Pandya AM. Genetics, X linked Inheritance. In: StatPearls. Treasure Island (FL): StatPearls Publishing: May 21, 2020


