
Case Report | DOI: https://doi.org/10.58489/2836-5917/015
1Nephrology Department, BP - A Beneficência Portuguesa de São Paulo, São Paulo, Brazil
2Intensive Care Unit, BP - A Beneficência Portuguesa de São Paulo, São Paulo, Brazil
*Corresponding Author: Tania Leme da Rocha Martinez,*
Citation: Tania Leme da Rocha Martinez, André Luis Valera Gasparoto, Ana Paula Pantoja Margeotto, Tereza Luiza Bellincanta Fakhouri, Anita L R Saldanha, Familial Chylomicronemia Syndrome 2(3). DOI: 10.58489/2836-5917/015
Copyright: © 2023 Tania Leme da Rocha Martinez, this is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 August 2023 | Accepted: 09 September 2023 | Published: 13 September 2023
Keywords: Familial Chylomicronemia Syndrome, Triglycerides, Genetic Analysis, Pancreatitis, Family history
Familial Chylomicronemia Syndrome is a severe and very rare metabolic disease characterized by chylomicronemia associated with recurrent episodes of abdominal pain and/or pancreatitis. The worldwide estimate is that Familial Chylomicronemia Syndrome occurs in one for every 500,000 to 1,000,000 people. It often manifests in childhood or adolescence and has been described in all ethnicities, with higher prevalence in some geographic areas, such as Quebec, due to the founder effect. Male patient, 40 years old, accountant, married, father of two daughters (1 and 4 years). Since the age of four, he knows how to have very high triglyceride values by warning from the laboratory. Genetic analysis confirmed deficiency of lipoprotein lipase. Pediatricians recommended the dietary and exercise lifestyle. As a teenager, he had pancreatitis when triglyceride levels reached 5,000 mg/dL. The patient does not present cardiovascular risk factors. We were wanted about three years ago when a second sister with the same condition died. It is noteworthy that his parents are first cousins. After therapeutic trials, little benefit was noticed. In association with the direction of hematology, we began to prescribe weekly and later biweekly dialysis. Since the emergence of volanesorsena, we have been prescribing it. Although its use in this patient is recent, six months, the results showed an important and significant reduction.
Familial Chylomicronemia Syndrome is a severe and very rare metabolic disease characterized by chylomicronemia associated with recurrent episodes of abdominal pain and/or pancreatitis. The worldwide estimate is that Familial Chylomicronemia Syndrome occurs at one in every 500,000 to 1,000,000 people. It often manifests itself in childhood or adolescence and has been described in all ethnicities, with higher prevalence in some geographic areas, such as Quebec, due to the founder effect [1,2,3].
Male patient, 40 years old, accountant, married, father of two daughters (1 and 4 years). Since the age of four, he knows how to have very high triglyceride values by warning from the laboratory. Pediatricians recommend a dietary and exercise lifestyle. As a teenager, he had pancreatitis when
triglyceride levels reached 5,000 mg/dL. At this time, one of his sisters died in a second pancreatitis [4] which had values similar to his own. It is noteworthy that his parents are first cousins. From the age of 19, he was treated in university services as well as his father as well as his other sister, maintaining levels of the order of 500 mg/dL with treatment. His cardiac propedeutics have always been and continue to be normal. The patient does not present cardiovascular risk factors. We were wanted about three years ago when a second sister with the same condition died. After therapeutic trials, little benefit was noticed. In association with the direction of hematology, we began to prescribe weekly and later biweekly dialysis. Since the emergence of the Volanesorsen, we have been prescribing it. There were no side effects observed except for a two-day painless erythema on the site of the injection.
Diagnosis: Lipoprotein lipase deficiency (OMIM # 238600) (Table 1).
Table 1. Genetic analysis. Pancreatitis panel.
Gene | Position | Variation | Consequence | Copies |
|
LPL | chr8:19.813.420 | G>T | p. Glu282* ENST00000650287 | Heterozygous (1 copy) | 5 |
LPL | chr8:19.811.790 | C>T | p. Pro234Leu ENST00000650287 | Heterozygous (1 copy) | 5 |
5 Definitely pathogenic
Genes analyzed: APOA5 APOC2 CFTR CTRC GPIHBP1 LMF1 LPL PRSS1 SPINK1
The evolutionary reports, adverse reactions and genetic examination are shown in Figures 1 to 4.
Patient adheres well to the low-fat diet and does physical activity regularly.
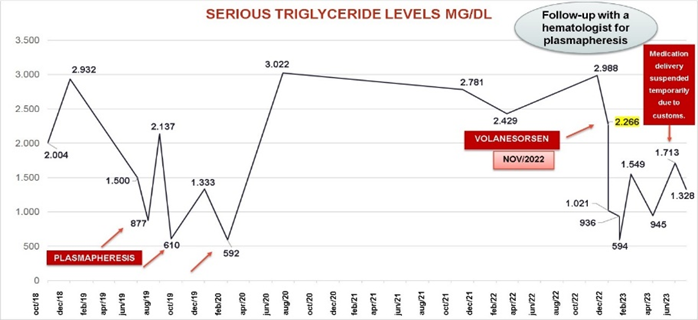
Figure 1. Plasmapheresis effects on triglycerides.
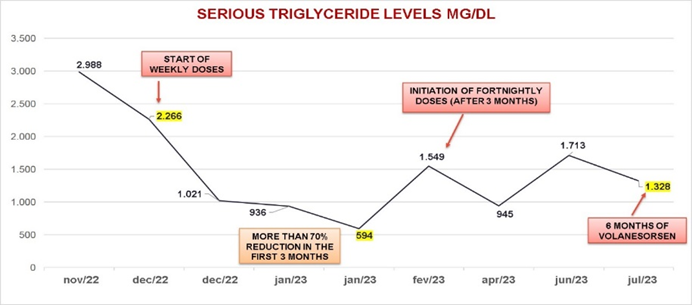
Figure 2. Effect of Volanesorsen on triglycerides.
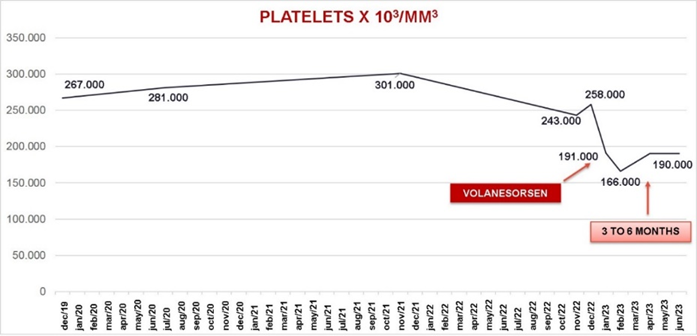
Figure 3. Platelets counts during observational period.

Figure 4. Painless erythema in the site of the injection for two days.
- A multidisciplinary team for the treatment of Familial Chylomicronemia Syndrome is essential.
- Adherence to diet and physical activity is essential for successful treatment.
- Urgency when treating: the patient's sister died in the second crisis of pancreatitis.
Poorly controlled triglycerides need to be treated.
None
None