Article In Press : Article / Volume 3, Issue 2
- CASE STUDY | DOI:
- https://doi.org/10.58489/2836-5127/021
Perineural Cysts of Tarlov: A Case Study
1Radiology Specialist, Radiology Department, Al-Namas General Hospital, Ministry of Health, Al-Namas City, Saudi Arabia.
Abdulwahab F. Alahmari *
Abdulwahab F. Alahmari. (2024). Perineural Cysts of Tarlov: A Case Study. Radiology Research and Diagnostic Imaging. 3(1); DOI: 10.58489/2836-5127/021
© 2024 Abdulwahab F. Alahmari, this is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- Received Date: 23-05-2024
- Accepted Date: 01-06-2024
- Published Date: 05-06-2024
Perineural Cyst; Cyst of Tarlov; Magnetic Resonance Imaging; Cervical Spine.
Abstract
This is a case of perineural cysts of Tarlov in a female patient who complains of having a chronic pain in the neck. An MRI scan was done which revealed a normal spine and vertebral column. Tiny bilateral perineural cysts were found on the MRI scan. This case study will gather all the information about the formation of perineural cysts of Tarlov, prevalence, appearance on MRI, associated conditions, and differential diagnosis.
Introduction
Tarlov cysts are CSF filled dilatations of the nerve root sheath at the dorsal root ganglia and they are common in the lumbosacral spine. On MRI of the lumber spine, they are seen on the sagittal sections behind the vertebra in the lumbosacral spine area and on para-sagittal sections (i.e. besides or lateral to) the cervical spine. On axial MRI sections, the cyst appears anterior oblique to the cervical spine and posterior to the lumbosacral spine. The cysts of Tarlov are extradural cysts, but they contain neural tissue which classified into a Nabors Type II meningeal cyst, whereas meningeal cyst is Type I Nabors cyst and spinal intrudural meningeal cyst is Type III Nabors cyst.
Cysts of Tarlov occur in 4.6% of the population and they affect women more [1]. Most of the perineural cysts are asymptomatic in 80% of the patients with cyst of tarlov. In another study, which shows that 15.59% of the tarlov cysts are symptomatic [2]. They are associated with 4 syndromes; Marfan syndrome, Ehlers-Danlos syndrome, Sjögren syndrome, and Loeys-Dietz syndrome. Most of the cases who have Tralov cysts, they are asymptomatic. The Tarlov cysts are common in the lumbosacral spine, but they can affect any part of the spine. The Tarlov cysts can be a simple cyst or complex loculated with septation mass. In symptomatic cases, aspiration of the cyst and injection of fibrin as a sealant to treat this medical condition is used. Other differential diagnoses are; dural ectasia, meningocele, cysticercosis, spinal synovial cyst, spinal metastases, and nerve sheath tumor.
Perineural cysts formation is still unknown, but there is a hypothesis by Tarlov indicating that trauma with subarachnoid hemorrhage make impairment of the veins that drainage the affected area then these veins raptured then a perineural cyst is formed. The perineural cysts have a one-way ball-valve which contributes in making compression on the spinal nerves in the affected area. This ball-valve make the perineural cyst to grow and compress the spinal nerves. Perineural cysts can be uni-loculated or multi-loculated. The MRI will show a thin walled cyst which is the perineural cyst.
Case Presentation
A 58-year-old female patient complaining of a pain in the neck and numbness in her upper limbs. An MRI scan of the neck was requested for her. The MRI scan showed a normal spine and vertebral column see (Figs. 1 and 2). The only finding that were seen are tiny perineural cysts on both sides.
Explanation of Formation
It could be an anatomical congenital anomaly as a dilatation in the spinal meninges that filled with CSF then with CSF high pressure might cause forming of a one-way valve that causes compression on the surrounding spinal nerves. Because the Tarlov theory about perineural cysts is not seen in most of the cases. Not all cases of perineural cysts have a history of subarachnoid hemorrhage or trauma.
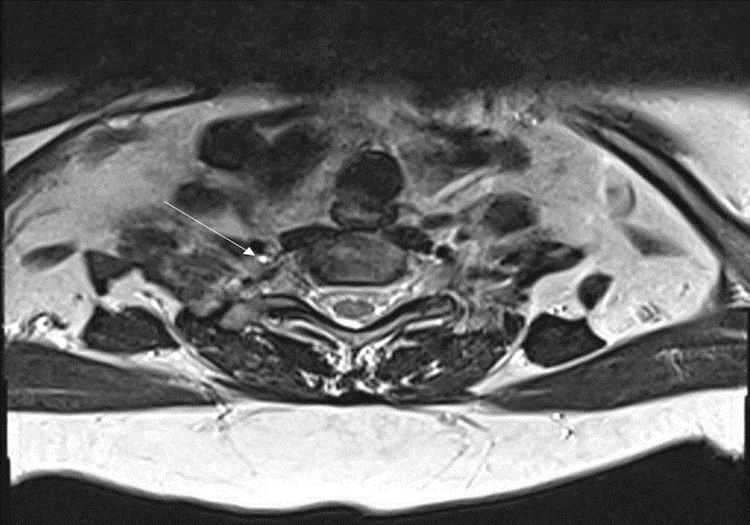
Fig 1: An axial MRI T2 shows a high intensity on the right anterior oblique side of the vertebra at the root of the spinal nerve which indicates a perineural cyst of Tarlov (white arrow).
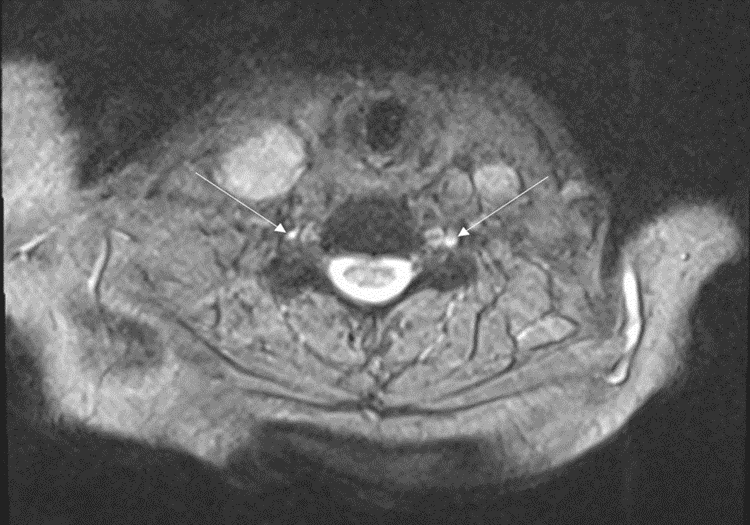
Fig 2:An axial MRI T2 shows bilateral perineural cysts of Tarlov on both sides (white arrows).
Discussion
Tarlov found these cysts on an autopsy in 1938 and he described three criteria to distinguish perineural cysts from meningeal cysts which are: 1) perineural cysts does not communicates with the spinal subarachnoid space (this criteria was found wrong because Tarlov cysts communicates with the spinal subarachnoid space, but the filling test on myelography shows the meningeal cysts fill immediately, while Tarlov cysts fill delayed, 2) a cyst of Tarlov affects at the dorsal nerve ganglion, the distal part of the dorsal nerve root, or the dorsal nerve ganglion, whereas a meningeal cyst affects the proximal part to the dorsal nerve ganglion, and 3) a cyst of Tarlov composed of nerve fibers or ganglion, while a meningeal cyst does contain any neural tissue.
Conclusion
Perineural cyst of Tarlov is common in the lumbosacral area and less common in the cervical region. It affects females more than males and it is symptomatic in 10% of the cases at least. To be diagnosed as a cyst of Tarlov, there are criteria to be fulfilled. The best imaging modality that can help in diagnosing this condition are MRI and myelography.
References
- Andrieux, C., Poglia, P., & Laudato, P. (2017). Tarlov cyst: a diagnostic of exclusion. International journal of surgery case reports, 39, 25-28.
- Klepinowski, T., Orbik, W., & Sagan, L. (2021). Global incidence of spinal perineural Tarlov’s cysts and their morphological characteristics: a meta-analysis of 13,266 subjects. Surgical and Radiologic Anatomy, 43, 855-863.


