Article In Press : Article / Volume 3, Issue 1
Case Report | DOI: https://doi.org/.
Noncompliance to Standard Treatment Procedures for Cancer Propelling Increase in the Mortality Rate of Cancer Patients in Benue State, Nigeria
- Consultant Oncologist/Lecturer: Federal University of Health Science Otukpo, Benue State-Nigeria
- Clinical Psychologist; Department of Oncology and Palliative Care, Federal Medical Centre Makurdi, Benue State-Nigeria
- Consultant Family Physician; Department of Family Medicine, Federal Medical Centre Makurdi, Benue Sate-Nigeria
- Clinical Psychologist; Branas Isaf-Care Tech Group, United Kingdom
- Radiation Oncologist; Faculty of Allied Health Sciences, Baze University Abuja-Nigeria
Correspondng Author: Samuel Anaja Otene
Citation: Samuel Anaja Otene, Ransome Msughve Labe, Laadi Terrumun Swende, Samuel Terkura Njor, Olayinka Benjamin Popoola. (2024). Noncompliance to Standard Treatment Procedures for Cancer Propelling Increase in the Mortality Rate of Cancer Patients in Benue State, Nigeria. Cancer Research and Cell Development. 3(1);
Copyright: © 2024 Samuel Anaja Otene, this is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received Date: 2024-03-25, Received Date: 2024-03-25, Published Date: 2024-04-12
Abstract Keywords: Noncompliance, Standard Treatment Procedures, Cancer, Mortality Rate Cancer Patients
Abstract
The purpose of this study was to gather, present, describe and explain the data on noncompliance to standard treatment procedures and its implication on increase in the mortality rate of cancer patients in Benue State. The study was a descriptive research and the data was obtained from the cancer patients case folders in the Record unit of the Oncology and Palliative Care Clinic Federal Medical Centre Makurdi. A total of 430 case folders of patients who received chemotherapy were thoroughly reviewed to analyze their level of compliance to cancer treatment procedures. Findings showed 53 different types of cancers diagnosed in the male and female patients but commonly were breast cancer 115(26.7%), cervical cancer 89(20.7%), liver cancer 19(4.4%), ovarian cancer, 16(3.7%), colorectal cancer 15(3.5%), Non-Hodgkin lymphoma cancer 15(3.5%), nasopharyngeal cancer 11(2.6%). Cervical cancer 16(18.0%), and breast cancer patients 7(6. 1%), were cancers diagnosed in patients with HIV status. Diagnosed cancer stages in patients was; stage I cancer 2.6%, stage II 46.7%, stage III 49.1% and stage IV 1.3%. Regarding compliance to treatment, 77.5% of cancer patients received chemotherapy, 13.5% surgery and 9.1%. went for radiative therapy. These findings corresponded with previous studies about noncompliance to cancer treatment procedures and increased patientsâ mortality. Unfortunately, poverty was found as the reason incapacitating cancer patientâs financial strength to full compliance to cancer treatment procedures. Thus, it will be appropriate for the Federal and States governments to budget and make specific funds available to support cancer patients to access their treatment requirements with ease.
Introduction
From the published Global cancer statistics (2020) Report, Sung et al (2021) projected that there are 19.3 million of cancer cases around the world. Apart from that huge global cancer estimation report, the International Agency for Research on Cancer [2] published a startling report that predicts a 77% increase in the global cancer cases by the year 2050. The report further revealed that 1-in-5 people develop cancer in their lifetime and 1-in-9 men and 1-in-12 women die from the disease. Relatedly, cancer is identified as the second leading cause of death worldwide, thus accounting for an estimated 10 million deaths, or nearly one in six deaths [3]. The rapid increase in the incidence of affliction with cancer worldwide cannot be overemphasized. This projection and the calculated rate of the prevalence of cancer among men and women cannot be doubted because of the observed evidence of the development of cancer among people in Benue State, Nigeria. Apparently, almost on a week basis people are diagnosed with cancer and referred for chemotherapy in the Department of Oncology and Palliative Care, Federal Medical Centre (FMC) Makurdi. In the clinic, between two to three new cancer patients are seen within a week; referred for chemotherapy from the specialist’s clinics in the FMC Makurdi or other hospitals within the State as well as the neighbouring States.
Additionally, but sadly, many of the patients referred for chemotherapy prior to surgery and after surgery came with a diagnosis of metastasized cancer, which doubtlessly depicts advanced-stage disease. This indicates that late presentation with the signs and symptoms of malignant tumour(s) is a common phenomenon among the people seeking medical care. The unfortunate reality of late presentation of cancer for treatment is that it leads to accelerated health deterioration, decreasing quality of life, and an increase in impending death of sufferers against the probable hope of survival. By the way, the National Cancer Control Plan [4] explained that cancer in Africa is characterized by late presentation, low access to treatment, and poor treatment outcomes. The burden of having and living with cancer by those afflicted with the disease has always been overwhelming to them in many untold ramifications. The experience of awful and disgraceful physical symptoms, agonizing pain and the waves of emotional distress triggered by a spectrum of psychosocial challenges such as poverty, and absence of a social network support to fall on, drags the patients gradually to the residence of death. Disturbing and problematic is the fact that many patients fall short of compliance to the recommended standard treatment procedures (e.g. chemotherapy surgery and radiation therapy). Indeed, the overwhelming burden of cancer associated with the psychosocial problems and poverty factors combine to frustrate and weakens the patients’ health, adjustment and ability to cope, leading to declining QOL and decreased chances of prolonged living, as they struggle with the life-threatening illness.
Literature Review
Situationally, the delay to access medical and possible curative treatment, and perhaps noncompliance to treatment directives due to financial constraints often makes the cancer patients appear like walking corpses who are awaiting execution. Vives (2022) explained that cancer is responsible for 72,000 deaths in Nigeria every year, with an estimated 102,000 new cases annually. Visibly, Vives observation cannot be disputed because many among those who are diagnosed with cancer usually do not have the financial capacity to access treatment for the disease aggressively. Consistent with this reality are findings from studies which have shown that lack of or delay of access to treatment, advanced stage presentation and noncompliance to recommended treatment processes or noncurative treatment for cancer is related to the reduction in the survival rate of cancer patients generally [6, 7, 8, 9,10, 11,12]. Even in cases whereby a cancer patient is determined and struggling to get treated, at some point his or her efforts faltered and adhering to treatment becomes difficult. Noncompliance to treatment refers to a patient who does not take a prescribed medication or follow a prescribed course of treatment [13]. According to Kleinsinger (2003), noncompliance is a situation whereby patients deviate significantly from most other patients (with similar medical problems) in degree of accepting and acting in accordance with medical advice, treatment recommendations, or follow-up in a way that directly or potentially jeopardizes their health or quality of life.
Other authors described non-compliance with treatment as the non-use or discontinuity of the treatment process and inattention or failure to follow the prescribed treatment by the patient. This means not taking medication, failure to modify lifestyle or diets, frequent changes in the treatment process, and failure to follow treatment directives or defectively performing the diagnostic tests, imaging, radiography, etc., are some examples of non-compliance with therapy [14.15,16]. Delays of cancer treatment occasioned by noncompliance to the recommended treatment directives typically and frequently leave room for disease reoccurrence, metastasis and progression to an advanced stage. The prime purpose of any prescribed treatment is to achieve desirable outcome from the planned care of patient seeking medical care. But irrespective of the best efforts of the medical doctors involved in the patients’ management, non-compliance is still a major problem that prevents the clinicians from achieving the expected therapeutic outcomes. Medical statistics showed that cancer is the second leading cause of mortality worldwide, accounting for an estimated 10 million deaths, or nearly one in six deaths [3] and this is explainable from the factors militating against patients’ strict compliance. Particularly, and unfortunately is the mortality incidence ratio of cancer for Nigeria when compared to others (especially more developed) Nations. For example, while in America, 19% of all breast cancer cases result in death, this percentage is 51% in Nigeria; tripling the rate seen in the US [4]. Same is with other people with other types of cancers.
Challenges Faced by Patients Diagnosed with Cancer Disease
The basic reasons behind patients’ delayed access to treatment and by extension noncompliance to the recommended treatment procedures is lack of finances to commence and sustain its treatment as they are informed to do. This inability is heightened by the miserable and precarious poverty situation that has become a common identity with the underprivilege population in Nigeria. Majority of the people afflicted with cancer in Nigeria are those who do not have the financial capacity to commence treatment for the cancer not to even mention strict adherence to it. For others, their struggling and staggering to comply with the treatment recommended stops at the stage of chemotherapy (which may be from four to eight cycles) and to some extent, surgery. Cancer treatment is unabatingly expensive and this is often typically beyond some patients to afford the least cost of one cycle of chemotherapy that could be between 40000 to 50000 naira, which is equivalent of 20 to 30 US dollars based on the current exchange rate. To add to the patients’ dilemma is the fact that the health and social welfare support system in Nigeria is abysmally ineffective and fundamentally out of reach for many cancer patients, especially for the underprivileged to benefit from it
The health insurance system in the country too is not reliable, and presently does not even offer comprehensive coverage for cancer care. Besides, the countless number of proliferated NGOs in the States of Nigeria are not doing enough to complement the governments developmental and social support programmes and welfare services to the needed population. Many NGOs are there representing the founder’s personal interest by swindling grants or funds obtained from foreign governments and international organizations and gives meagre financial assistance to a selective few they later used to doctor the data to show their spending of the funds received. This is confirmed from the reports in the available literatures that many of the NGOs with attractive names of foundation for this and that are faux and mushroom organizations existing as agents and routes for money laundering and treasurers of national or States development funds stolen by politicians and top government officials [17,18,19,20,21]. Additionally, in 2017, Okonjo Iweala stated that some corrupt politicians were setting up NGOs to cover up their deeds. As a matter of fact, cancer patients Nigeria with underprivileged background and without a support network are suffering and living with their illness at the mercy of fate. This is because many cancer patients commenced treatment but stops midway and not go farther because they did not have money anywhere to bear the costs involved to complete the treatments recommended. Constrained by the challenges of the illness and finances with no help from anyone in a precarious poverty-stricken society, dying early from cancer is a common occurrence among those afflicted with the disease in Benue State. In view of this observed situation, this study focused on obtaining and describing the data about patients’ noncompliance to standard treatment procedures for cancer propelling increase in the mortality rate against the expectation and hope of their survivorship or minimization of early death.
Aim and Objectives of the Study
Economically, most cancer patients are frequently in financially difficult situation that disable their wish and willingness for compliance to all the treatment procedures. Consequently, the purpose of this study was to obtain, describe and explain in statistical form the data on the cancer patients’ noncompliance to standard treatment procedures as evidence for the increase in death from cancer illness. The objectives of the study are to:
- Describe the number of diagnosed cancer cases from 2013-2022 in Federal Medical Centre Makurdi.
- Describe the types of cancers people are diagnosed to have in Benue State.
- To identify and discuss the types of cancer diagnosed in people with positive retroviral/HIV status.
- Identify and discuss the stages of cancer presented by patients on entry in the hospital for treatment.
- Describe cancer patient’s noncompliance to standard treatment procedures and its indication for increase of the mortality rate in Benue State.
Research Questions
- To what extent does cancer cases increase in the population of Benue State?
- What are the types of cancers people are diagnosed to have in Benue State?
- What are the types of cancer that are mostly diagnosed in people with positive retroviral/HIV status in Benue State?
- At what stages did patients present cancer in the hospital for treatment in Benue State?
- What aspects of standard treatment procedures are cancer patients usually noncompliant with, leading to predictable death and increased mortality rate in Benue State?
Method
Research design
The study adopted a descriptive design with the aim of describing and explaining the implication of noncompliance to standard treatment procedures propelling increase in mortality rate rather than decreasing it among the people who are diagnosed with cancer, a life-threatening disease. The description of this disturbing phenomenon was done in ways that reflect a clear and comprehensive picture of the physical, and socioeconomic challenges militating against the treatment of patients’ cancer and achievement of the expected outcome desired by both the healthcare professionals and patients.
Method of Data Collection
The data related to the study was obtained in two methods, which include interview with patients and review of documented histories in their case folders on referral for chemotherapy in Oncology and Palliative Care clinic Federal Medical Centre Makurdi. The primary information required and obtained was on patient’s sex, age, marital status, tribe, type of cancer diagnosed, stage of cancer at time of diagnosis, retroviral status (RVST), treatment received (e.g. chemotherapy, surgery and radiotherapy). In addition to obtaining data from the patients’ case folders, other information on the reasons that are frustrating patient’s inability to be compliant to the standard treatment procedures (chemotherapy, surgery and radiation therapy) recommended to them as a cancer diagnosis is established from histopathology investigation result was acquired through oral conversation with the patient in the clinic.
Data Analysis
The data was statistically analyze using primarily frequency and percentages, which makes easier for presentation and vivid description of the findings. The analysis was done with the use of SPSS version .20 and the results were presented in tables, histograms and graphic charts.
Results
The results of the study were derived from the analysis of the data obtained in the medical records of the patients that were receiving chemotherapy the Oncology and palliative Clinic of the hospital. Therefore, the findings are presented and interpreted as it is represented on the tables, histograms and pie chart,
Table 1: Sociodemographic characteristics of sample (cancer patients) (n=430)
| Variables | Frequency | Percent |
| Age | ||
| <20> | 10 | 2.3 |
| 20-30 | 56 | 13.0 |
| 31-40 | 92 | 21.4 |
| 41-50 | 105 | 24.4 |
| >51 | 167 | 38.8 |
| Mean=46.74±14.52 | ||
| Sex | ||
| Male | 125 | 29.1 |
| Female | 305 | 70.9 |
| Marital Status (n=419) | ||
| Married | 345 | 82.3 |
| Single | 73 | 17.4 |
| Widowed | 1 | 0.2 |
| Tribe | ||
| Tiv | 260 | 60.5 |
| Idoma | 100 | 23.3 |
| Igede | 10 | 2.3 |
| Others | 60 | 14.0 |
Table 1 above represented the sociodemographic characteristics of cancer patients that were receiving chemotherapy and other palliatives care services from 2013 to July, 2023. They were 586 cancer patients registered for treatment on referral for chemotherapy from the GOPD, SOPD and other health facilities within Benue State and neighbouring States. However, 156 out 586 diagnosed with cancer and referred for chemotherapy left to never return to receive treatment because they were unable to afford the cost of any of the treatment procedure recommended. Those that were able to manage to receive chemotherapy and have surgery were 305(70.9%) females and 129(21.9%) men. The patients whose documented treatment histories were analyzed comprised of Tiv, Idoma, Igede and other tribes that were either indigenous or nonindigenous citizens.
Table 2: Distribution of types of cancers diagnosed in patients (N=430)
| Variable | Frequency | Percent |
|---|---|---|
| BREAST CANCER | 115 | 26.7 |
| CERVICAL CANCER | 89 | 20.7 |
| COLORECTAL CANCER | 22 | 5.1 |
| LIVER CANCER | 19 | 4.4 |
| OVARIAN CANCER | 16 | 3.7 |
| NON-HODGKIN’S LYMPHOMA | 15 | 3.5 |
| PROSTATE CANCER | 13 | 3.1 |
| RHABDOMYOSARCOMA | 13 | 3.1 |
| NASOPHARYNGEAL CANCER | 11 | 2.6 |
| MELANOMA | 9 | 2.1 |
| LUNG CANCER | 8 | 2.0 |
| BLADDER CANCER | 6 | 1.5 |
| KAPOSISARCOMA | 6 | 1.5 |
| NON-MELANOMA SKIN CANCER | 6 | 1.5 |
| ENDOMETRIAL CANCER | 5 | 1.3 |
| TONGUE CANCER | 5 | 1.3 |
| GASTRO-INTESTINAL STROMAL TUMOUR | 4 | 0.9 |
| OESOPHAGEAL CANCER | 4 | 0.9 |
| ORAL MUCOSA CANCER | 4 | 0.9 |
| FIBROSARCOMA | 3 | 0.7 |
| TESTICULAR SEMINOMAS | 3 | 0.7 |
| PLEOMORPHIC SARCOMA | 3 | 0.7 |
| CHORIOCARCINOMA | 3 | 0.7 |
| LIPOSARCOMA | 3 | 0.7 |
| GASTRIC CANCER | 3 | 0.7 |
| ORBITAL SQUAMOUS CELL CARCINOMA | 3 | 0.7 |
| MAXILLARY SINUS CANCER | 3 | 0.7 |
| THYMOMA | 3 | 0.7 |
| CHONDROSARCOMA | 2 | 0.5 |
| UTERINE LEIOMYSARCOMAOMA | 2 | 0.5 |
| LEUKAEMIA | 2 | 0.5 |
| LYMPHOSARCOMA | 2 | 0.5 |
| PANCREATIC CANCER | 2 | 0.5 |
| NASAL CAVITY SQUAMOUS CELL CANCER | 2 | 0.5 |
| AURICULAR CANCER | 2 | 0.5 |
| CANCER OF UNKNOWN PRIMARY | 2 | 0.5 |
| LARYNGEAL CANCER | 1 | 0.2 |
| OVARIAN TERATOMA | 1 | 0.2 |
| BRAIN CANCER | 1 | 0.2 |
| MALIGNANT PERIPHERAL NERVE SHEATH TUMOR | 1 | 0.2 |
| URETHRAL CANCER | 1 | 0.2 |
| RETINAL CANCER | 1 | 0.2 |
| MAXILLOFACIAL CANCER | 1 | 0.2 |
| PLASMAYTOMA | 1 | 0.2 |
| SSC SCROTUM | 1 | 0.2 |
| RETINOBLASTOMA | 1 | 0.2 |
| VULVA CANCER | 1 | 0.2 |
| HODGKIN’S LYMPHOMA | 1 | 0.2 |
| ANGIOSARCOMA | 1 | 0.2 |
| NEPHROBLASTOMA | 1 | 0.2 |
| OLFACTORY NEUROMA | 1 | 0.2 |
| OROPHARYNGEAL CANCER | 1 | 0.2 |
| NEUROFIBROMATOSIS | 1 | 0.2 |
Source: Records Unit, Oncology and Palliative Clinic FMC Makurdi,
Table 2 above represents the description of 53 types of cancer cases that are diagnosed and referred for chemotherapy in Oncology and Palliative Care Clinic FMC, Makurdi in Benue State. Commonest and highest number of the cancers seen diagnosed in the patients are breast cancer 115(26.7%), cervical cancer 89(20.7%), colorectal cancer 22(5.1%), liver cancer 19(4.4%), ovarian cancer, 16(3.7%), prostate cancer 15(3.5%), Non-Hodgkin lymphoma cancer 15(3.5%), rhabdomyosarcoma 13(3.1%), nasopharyngeal cancer 11(2.6%) and many others.
Table 3: Distribution of types of cancer diagnosed in patients with HIV status
Positive n=41 n (%) | Negative n=389 n (%) | ||
|---|---|---|---|
| TYPES OF CANCERS | HIV STATUS | ||
| Breast Cancer | 7(6.1) | 108(93.9) | |
| Cervical Cancer | 16(18.0) | 73(82.0) | |
| Colorectal Cancer | 1(4.5) | 21(95.5) | |
| Liver Cancer | 0(0.0) | 19(100.0) | |
| Ovarian Cancer | 0(0.0) | 16(100.0) | |
| Non-Hodgkin’s Lymphoma | 2(13.3) | 13(86.7) | |
| Prostate Cancer | 2(15.4) | 11(84.6) | |
| Rhabdomyosarcoma | 0(0.0) | 13(100.0) | |
| Nasopharyngeal Cancer | 1(9.0) | 10(91.0) | |
| Melanoma | 0(0.0) | 9(100.0) | |
| Lung Cancer | 0(0.0) | 8(100.0) | |
| Bladder Cancer | 0(0.0) | 6(100.0) | |
| Kaposi Sarcoma | 4(66.7) | 2(33.3) | |
| Non-Melanoma Skin Cancer | 0(0.0) | 6(100.0) | |
| Endometrial Cancer | 0(0.0) | 5(100.0) | |
| Tongue Cancer | 1(20.0) | 4(80.0) | |
| Gastro-Intestinal Stromal Tumour | 0(0.0) | 4(100.0) | |
| Oesophageal Cancer | 1(25.0) | 3(75.0) | |
| Oral Mucosa Cancer | 0(0.0) | 4(100.0) | |
| Fibrosarcoma | 0(0.0) | 3(100.0) | |
| Testicular Seminoma | 0(0.0) | 3(100.0) | |
| Pleomorphic Sarcoma | 0(0.0) | 3(100.0) | |
| Choriocarcinoma | 0(0.0) | 3(100.0) | |
| Liposarcoma | 1(33.3) | 2(66.7) | |
| Gastric Cancer | 0(0.0) | 3(100.0) | |
| Orbital Squamous Cell Carcinoma | 1(33.3) | 2(66.7) | |
| Maxillary Sinus Carcinoma | 0(0.0) | 3(100.0) | |
| Thymoma | 0(0.0) | 3(100.0) | |
| Chondrosarcoma | 0(0.0) | 2(100.0) | |
| Uterine Leiyomyosarcoma | 0(0.0) | 2(100.0) | |
| Leukaemia | 0(0.0) | 2(100.0) | |
| Lymphosarcoma | 1(50.0) | 1(50.0) | |
| Pancreatic Cancer | 0(0.0) | 2(100.0) | |
| Variables | Cont. | Cont. | |
| Nasal Cavity Squamous Cell Carcinoma | 0(0.0) | 2(100.0) | |
| Auricular Cancer | 0(0.0) | 2(100.0) | |
| Cancer of Unknown Primary | 0(0.0) | 2(100.0) | |
| Laryngeal Cancer | 0(0.0) | 1(100.0) | |
| Ovarian Teratoma | 0(0.0) | 1(100.0) | |
| Brain Cancer | 0(0.0) | 1(100.0) | |
| Malignant Peripheral Nerve Sheath Tumour | 0(0.0) | 1(100.0) | |
| Urethral Cancer | 0(0.0) | 1(100.0) | |
| Retinal Cancer | 0(0.0) | 1(100.0) | |
| Maxillofacial Cancer | 0(0.0) | 1(100.0) | |
| Plasmacytoma | 1(100.0) | 0(0.0) | |
| Scrotal Squamous Cell Carcinoma | 1(100.0) | 0(0.0) | |
| Retinoblastoma | 0(0.0) | 1(100.0) | |
| Vulva Cancer | 1(100.0) | 0(0.0) | |
| Hodgkin’s Lymphoma | 0(0.0) | 1(100.0) | |
| Angiosarcoma | 0(0.0) | 1(100.0) | |
| Nephroblastoma | 0(0.0) | 1(100.0) | |
| Olfactory Neuroma | 0(0.0) | 1(100.0) | |
| Oropharyngeal Cancer | 0(0.0) | 1(100.0) | |
| Neurofibromatosis | 0(0.0) | 1(100.0) | |
Table 3 shows the types of cancers diagnosed in patients with retroviral or HIV status. Among the cancers were cervical cancer patients 16(18.0%), breast cancer patients 7(6. 1%), Kaposi sarcoma 4(66.7%), prostate cancer 2 (15.4%) and Non-Hodgkin’s Lymphoma 2(13.3%) and a few others.
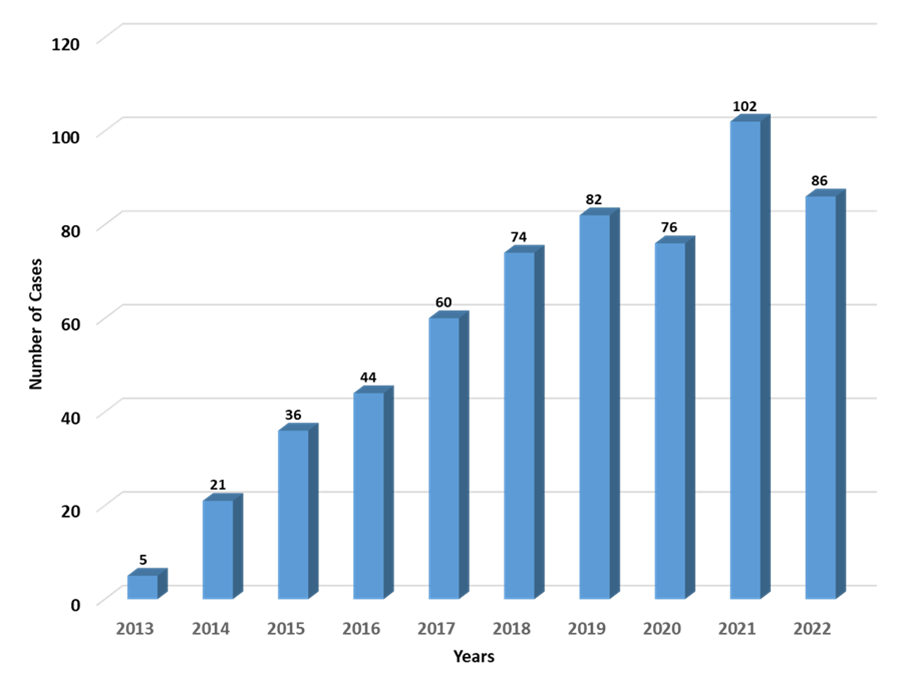
The bar chart shows a galloping increase in the cases of cancer diagnosed in the people in Benue State. The data obtained to produce these statistics was collected beginning from 2013, the year the oncology and palliative care services was set up in FMC Makurdi.
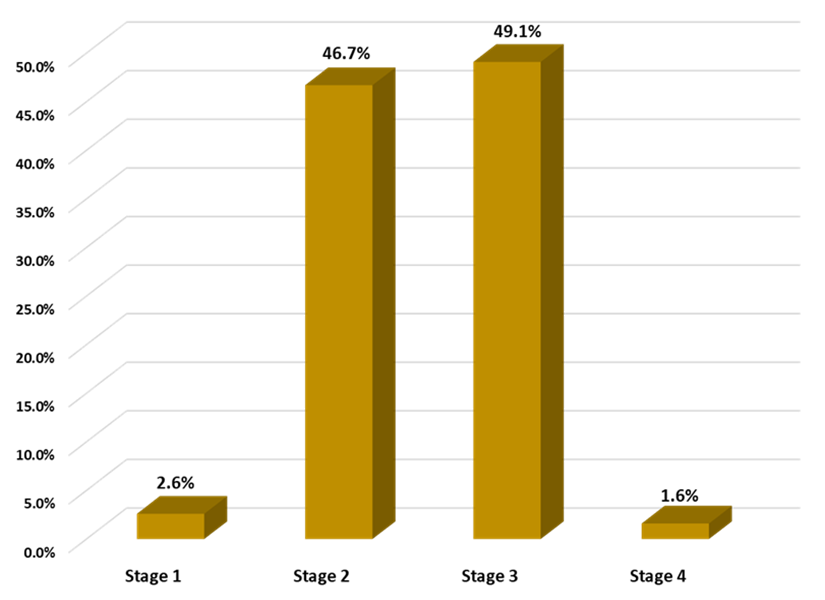
The bar charts above represents the total percentages of stages of cancer diagnosed in patients from the histopathology result. Patients presenting with stage I cancer 2.6%, stage II 46.7%, stage III 49.1% and stage IV 1.3%. The findings showed that people who had signs and symptoms as evidence of cancer in their body presented late for medical treatment.
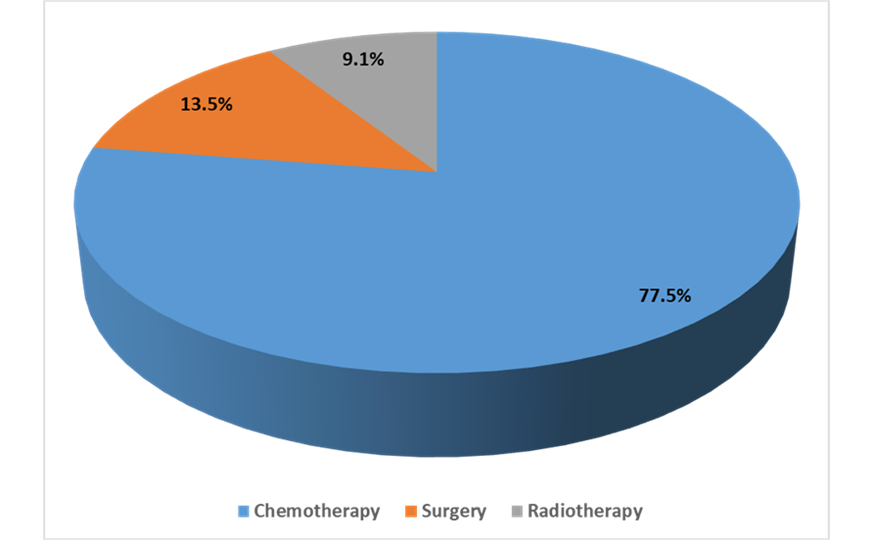
The pie chart above shows the percentage level of cancer patients’ compliance to the recommended standard treatment procedures to the disease. Accordingly, 77.5% of cancer patients shows compliance to chemotherapy, 13.5% had the required surgery either before or after chemotherapy, and 9.1%. were able to go for the recommended radiotherapy to complete the three stages of treatment.
Discussion
The persistent rise in the cases of cancer in Benue State and in Nigeria as a whole cannot be overemphasized. Unfortunately, the rapid and high increase of the disease is almost matching with the higher death rate from the disease as reported by [2,22, 4, 5, 3]. It is medically recognized that the risk of dying soon from cancer has been greatly reduced in the 21st century in most countries in the world due to the use of new scientific advancements in anticancer drugs and inventions of treatment methods. Cohen (2023) explained that, this development has led to an unprecedented progress in the survival from cancer as more people than ever are surviving the disease. Cancer treatment involves the use of chemotherapy alone or adoption of a triple treatment approaches which include chemotherapy, surgery and radiation therapy. However, compliance with these recognized standard treatment procedures for many diagnosed with the disease in Benue State is a major challenge. First and foremost, many people who present late with cancer for treatment, do not know it is cancer at the onset of manifestation of symptoms of the disease. Consequently, their first reaction to a noticeable unusual and disturbing abnormal growth or symptom of illness is to seek treatment from traditional medicine practitioners/herbalists on their own decision or on the advice of family members and friends.
The subsequent decision to seek medical help is made when the person finds that he or she is not getting healed and the tumour growth and symptoms are progressing uncontrollably. Others in many cases seeks treatment from private hospitals within their locality, (community or town). Largely, these private hospital facilities do not have the required laboratory equipment for proper investigation (including biopsy and Histopathology) to determine accurately the nature and type of disease the patient is presenting with. Therefore, the treatment decision for surgical removal of the tumour in a patient with, for example, cervical or breast cancer signs and symptoms is premised on the assumption or suspicion that it is a fibroid growth, or an ordinary lump in the breast, respectively. Apparently, within a limited period after the surgery is performed, the patient feels relieved and satisfied that their problem is cured as the symptoms are mitigated. However, after some months or years, the growth recurs or there will be an emerging swelling in the affected organ.
By virtue of the observed incidence of cancer and patients’ challenges in accessing treatment as expected, this study was conceived and carried out with the sole aim to provide a comprehensive and reliable evidence-based information about the persistent increase in the cases of cancer in Benue State. And to also explain the patients’ pervasive noncompliance to standard treatment procedures which is propelling increase in the mortality from the disease. Research questions which were asked are discussed following the findings obtained from the analysis of the data collected.
Question One: To what extent does cancer cases increase in the population of Benue State?
The increase in the cases of cancer, a recognized life-threatening illness is both a national and global concern as reported by [2,5,3]. Evidently, this has been reliably established in the Benue State from this study based on the data obtained in the Oncology and Palliative Care Clinic Federal Medical Centre Makurdi record unit. The oncology and palliative care department/clinic was setup in 2013 for the purpose of providing curative and palliative care intervention to patients with cancer. As presented on the bar chart in figure I, the clinic started intervention with five cancer patients. From this small number, the number of referrals began to increase from GOPD, SOPD/clinics in the hospital and other health facilities in the State 2014 forward (see figure I). The rise in the record of the cancer cases in the Benue State population is a proof of previous statistical reports by other researchers regarding the rise in the cases of cancers in other States in Nigeria [22,24,5].
Question Two: What are the types of cancers that are diagnosed in the Benue State population?
Cancer can develop in any part of the body excluding the hairs and nails irrespective of the individual’s sex identity, age and socioeconomic status. As a result of its unsparing growth in any part of a person body system, there are many types of cancers with different medical names based on which part of the body they developed from, or what particular type of cell they originate from. Invariably, the findings from the documented history of the cancer patients have revealed this to each patient’s diagnosis. This shows that the total number of 53 cancers the people are diagnosed with in Benue State comprised of cancers that falls within international classification of cancers groups like carcinomas, sarcomas, leukaemia, lymphomas and myeloma, brain and spinal cord [25,26,4,3].
Question Three: What are the types of cancers that are mostly diagnosed in people with positive retroviral/HIV status?
Cancer has causes that are known to be related to controllable and uncontrollable factors. According to WHO (2022) cancer occurs as a result of changes in normal body cells, transforming into abnormal cells via a multistage process that eventually progresses to frank malignancy. The transformation of these cells is triggered by the interaction between the individual genetic predisposition and three primary external agents. These external agents are the physical carcinogens like ultraviolet and ionizing radiation; chemical carcinogens ingested from tobacco, alcohol, aflatoxin and arsenic drinks and biological carcinogens comprising of infections from particular viruses, bacteria and parasites [3]. Relatedly, this study found that cervical cancer 18% is the highest cancer that patients with positive retroviral/HIV status (related biological carcinogens) are typically diagnosed to have. Incidentally, 6.1% of breast cancer patients were also noticed to be HIV-positive, making breast cancer second to cervical cancer, Kaposi sarcoma, a HIV-related cancer 66.7%, and other cancers diagnosed in patients with positive HIV status are also shown (see table 3). This finding has supported the other studies that had found and established the link between cervical cancer with women with HIV status. Arithmetically, these studies have shown that women with HIV are six times more susceptible to develop cervical cancer more than those without HIV [27,28,29,30,31,32]. Disturbingly, it is reported that eighty to eighty-five percent of cases of cervical cancer are women from developing countries in the sub-Sahara region [32] including Nigeria along with her thirty-six States. Moreover, HIV is known to be 5% contributing cause in all cases of cervical cancer.
Question Four: At what stages do patients presented with cancer in the hospital for treatment in Benue State?
Understandably, Nigeria is a developing country and a country with the largest population living in a dismal state of poverty. Due to this high abject poverty experience in the country, many people who later seek medical treatment presented an advanced stage disease condition. This is evident from the findings of this study as represented on figure 3 revealing that 46.7% of cancer presented at stage II, 49,1% stage III and 1.6% stage IV and only 2.6% are came with Stage I cancer. In fact, for some people the ignorance leading them to use traditional medicine on noticing the development of the disease and, in some cases, the high cost of cancer treatment discouraged their early access to cancer screening, detection and intervention are the reasons for late presented. For others, the disease’s opportunity for rapid progression is as a result of their pseudo-belief in witchcraft role causing their development of the illness. Blinded by these reasons at the onset of manifestation of the disease, by the time they leave the traditional medicine providers to seek medical care, a reasonable part of money they may have was expended on paying exorbitant charges for treatment to herbalist and the disease may have metastasized or advanced to an incurable stage. Unfortunately, for those who left the herbalists, no longer have sufficient financial resources when they entered the hospitals where they received a cancer diagnosis. As a result, they usually commenced treatments but end up wobbling with compliance to treatment directives. Many people with low or no income in many cases at this point opt to borrowing money from people, selling their properties, and others go about soliciting for money from individuals and groups to buy their anticancer drugs or pay for treatment. Access to treatment for people diagnosed with cancer in Benue State is completely low and this is compounded by poverty with their out-of-pocket sponsor of treatment is frankly limited. Many diagnosed with cancer, due to their underprivileged status and dismal financial background are always heard lamenting about financial constraints from the first day of coming to the clinic on referral for chemotherapy. In some cases, some patients go back home and never return to undertake the treatment procedures (chemotherapy, surgery, and radiotherapy) recommended to them. According to Coker (n.d.) the gap still remains wide to bridge for people access to cancer treatment in the country.
Recognizing that cancer treatment is very expensive and payment for it for many patients is usually out-of-pocket [16], the patients are all the time lamenting about financial constraints frustrating their adherence to treatment recommended. This constantly represents a reason for an easy conclusion that they will be unable to commence and continue treatment to the already advanced stage disease. While other countries are providing access to the latest invented cancer drugs and subsidize treatment through public insurance schemes, cancer patients in Nigeria are seen struggle and sweating to purchase basic chemotherapy drugs. Besides, the experience of financial problems, patients’ noncompliance to treatments is heightened by the unbearable rise in the cost of transportation and increases in the cost of drugs due to the president Ahmed Bola Tinubu new government thoughtless harsh economic recovery policy of subsidy removal, and floating of the naira for exchange rate. The experience of financial problems by patients primarily because of financial difficulties tend to impact negatively on their health and lives, due to noncompliance standard treatment procedures [34,35,36].
Question Five: What aspect(s) of standard treatment procedures cancer patients are usually noncompliant to undertake that leading to predictable death and increased mortality rate in Benue State?
Noncompliance to treatment directives is a commonly observed among patients seeking medical care. Patients inconsistent response to the culture of adherence and compliance to doctors’ information on recommended process of treatment frequently interfered with the planned treatment approach, prolong duration of intervention, delay the expected outcome and even give an opportunity for disease progression. This in some cases results to death due to uncontrollable cancer metastasis to incurable experience that pushes the patient to end-stage management status. This was evidently found from the analysis of the data that noncompliance to standard treatment procedures and propelling increase in the mortality of cancer patients in Benue State. As represented on the pie chart, the findings showed that from the records of 430 cancer patients reviewed, 77.5% of cancer patients showed their compliance to chemotherapy, 13.5% went for the surgery required either before or after chemotherapy and only 9.1% were able to go for the recommended radiotherapy.
Medically, the treatment of cancer involves a multimodal approach and radiotherapy plays the role for elimination of malignant tumours [34]. Basically, chemotherapy, surgery, radiotherapy are the three most common and necessary procedures required in the treatment of cancers. However, the finding in this study clearly revealed that cancer patients’ noncompliance to these triple treatment methods is a prevailing problem that is impeding the achievement of the expected outcomes in the management of their cancer illness. Therefore, it is reasonable to conclude that even though many cases of cancer are curable or can be effectively managed to save the individual, improve quality of life and minimize the chances of his or her early death but this is often not possible to achieve. Definitely, for patients who received chemotherapy and surgery but did not go forward for radiotherapy is part of noncompliance to standard treatment procedures. And the consequence will be fatal in the long run for those with cancer that required radiotherapy to complete the treatment process.
Ohri and Garg (2016) has previously emphasized that, missed radiation therapy sessions during cancer increased risk of their disease reoccurring. In fact, and unfortunately, cancer patients in Benue State have been dying within a short time of missed radiotherapy due to tumour reoccurrence, disease progression and cancer metastasis. Some of these patients, their death is reported back to our clinic, but for others, their families are unable to reach us with the news of the death of the patients. Largely, this finding explicitly supported the previous studies which have established that noncompliance to standard treatment procedures often leads to patients’ fatal outcome. For example, Kliensinger (2003) states that noncompliance behaviour frequently interferes with effectiveness of treatment for variety of medical conditions and can have serious consequences. Similarly, Palwe, Patil, Pandit and Nagaskar (2019) explained that delay or prolongation of treatment is associated with a relative risk of local reoccurrence by up to 2% per day for specific malignancies.
Declining radiotherapy is significantly contributing to diminish the survival rate of cancer patients in Benue State and across Nigeria. Evidence from previous studies have confirmed this observable problem of patients declining radiotherapy in different researches. For example, Umoke and Garba (2019) found that 46% of the 37 patients with advanced disease who required chemotherapy completed the prescribed six courses. None of the patients who required radiotherapy received it. Largely, Umoke and Garba stressed that late presentation, poor compliance and adherence to treatment strategies, and poor access to adjuvant therapy were the major challenges to good outcome for this disease. Similarly, Vermeire, Hearnshaw, Van Royen, and Denekens, (2001) as cited in Naghavi et al., (2019) emphasize that due to patients’ noncompliance with therapy and their failure to report, diagnosis may become difficult for physicians; it adds to the complexity of treatment and results in waste of resources in the healthcare system. Ohri and Gard (2016) also states that noncompliance with radiation therapy may serve as a broader warning sign for additional risk factors that negatively affect the expected outcome. Joseph et al (2012) reported that 15427 women diagnosed with breast cancer showed that 185 (1.2%) patients refused standard treatment and the five-years survival rates were 43.2% for those who refused standard treatment and 81.9.% for those who received them. Hansen (2024) explained that nonadherence to treatment cancer leads to worse outcomes with frequent hospitalization, disease worsening, prolong recovery and increased mortality.
Noncompliance to treatment refers to a patient who does not take a prescribed medication or follow a prescribed planned treatment by the patient without consultation from the treating clinician (13, 39). According to Kliensinger (2003), Other authors described non-compliance with treatment as the non-use or discontinuity of the treatment process and inattention or failure to follow the prescribed treatment by the patient. This means not taking medication, failure to modify lifestyle or diets, frequent changes in the treatment process, and failure to follow or defectively perform the diagnostic tests, imaging, radiography, etc., are some examples of non-compliance with therapy [15,16] as cited in Naghavi, 2019). The primary aim of any prescribed cancer treatment procedures treatment is to achieve desirable outcome in a patient medical care. Non-compliance with prescribed treatment is an important cause of preventable mortality and economic burden [36]. But despite the concerted efforts of medical doctors in the hospital, patients’ non-compliance is still a major problem that prevents the clinicians to achieve the desired therapeutic outcomes for most of the cancer patients in Benue State.
Conclusion
Patients’ decision to decline or deferred other cancer treatment procedures may be difficult to accept when it is very obvious that the desired outcome of his or her treatment can only be achieved with the prompt application of the recommended treatment methods. However, the inability of most cancer patients to access and complete the required treatment recommended by the doctors in the hospital is a common noticeable problem that is prevailing among the patients and propelling the mortality rate from cancer. Actually, noncompliance is probably what some patients do not wish but because they are helplessly constrained by lack of money to go through all the treatment procedures (chemotherapy, surgery and radiotherapy). In fact, some patients even hardly have the money to afford purchase of the chemotherapy drugs or pay for surgery, not to talk of radiotherapy that is usually necessary but is obviously costly. Others managed to receive chemotherapy and/or have surgery (mastectomy, hysterectomy, prostatectomy etc.) depending on the type of cancer. But after these treatment methods, they willingly or unwillingly decided not to go further for radiotherapy, due largely to paucity of funds or perhaps due to personal believe and contentment with the transitory feeling of wellness.
Typically, many cancer patients frequently resort to declining radiotherapy probably due to financial difficulties or as a result of a pseudo-active conviction with the feeling of wellness after chemotherapy and surgery. But lack of money is generally the main reason for many patients because they are always pre-informed about the huge amount of money needed to access radiotherapy, which they instantly perceived as been beyond their capacity to afford. Understandably, the cost of radiotherapy varies depending on the place (State in Nigeria) of the radiotherapy centre and whether the application of radiotherapy is to be with a radical or palliative intent, but presumably the cost ranges from 750 thousand to above 1.7million naira. This is exclusive of many radiological and laboratory investigations required for close monitoring in the course of radiotherapy. By virtue of the high cost of cancer treatment and the patients’ lack of financial capacity to access it has been established as the reasons for their noncompliance as confirmed by Naghavi et al (2019) assertion that non-compliance with specialists’ orders include patient-related (patient-centered), disease-related, therapy-related, the healthcare provider related (healthcare system), and socioeconomic factors as the case may be.
Recommendations
- It is essential for the Federal and States governments to constantly budget and make specific funds available to support cancer patients to access their treatment requirements with ease.
- The government should subsidize the healthcare free of charge if not for all illnesses, at least for cancer disease in order to ease the burden of patients out-of-pocket financing of treatment bills for consultation, tests, admission, surgery, drugs and any other treatment procedures.
- The government both Federal and State should be magnanimous to implement the concept behind her renaming Ministry of Health and Social Welfare by enrolling individuals from the vulnerable population into its health insurance scheme as a way of supporting them on accessing treatment of their illnesses.
- The NGOs or cancer foundations in Benue State and Nigeria should step up their degree of responsibility towards humanitarian services with increased level feeling of empathy for people with cancer and support limitlessly their treatment from funds they periodically receive from governments and foreign individuals, groups or organizations.
- Cancer care providers should constantly give psycho-education and counselling to cancer patients to emphasize the need for strict adherence to standard treatment procedures and the associated consequences of declining compliance.
- The international organizations can come in to seek to have direct partnership with Federal Medical Centre Makurdi when they considered it necessary to extend their humanitarian support to the area of cancer management in Nigeria.
Acknowledgments
The successful completion of this study cannot be appraised without expression of gratitude to the role-played by authors at every stage of it. We are very grateful to the contributions of Emmanuel Ezenwajiaku a serving National Youth Service Corp in the department who helped in the obtaining of the data from the cancer patients case folders. We are also thankful to Tersoo Apaa whose statistical analytical knowledge and skills assisted in producing the SPSS-based results output which has served as the basis for which we have confidently reported the findings.
Funding
Actually, we did not receive any financial assistance from any individual or organizations facilitate the starting and completion of the study. It was mainly from the authors’ out-of-pocket contributions that was used at every stage of the study to produce the quality of the work we are happy to published.
Authors contributions to the study
Each author in the study made a significant contribution to the study that helped to it to a successful end. Accordingly, its conceptualization was by Labe, RM and Otene, AS; Methodology, Labe, RM, Otene, AS, Swende, LT. and Popoola, OB; Data Collection, Labe, RM and Emmanuel Ezenwajiaku; Data Analysis, Terssoo Apaa; Resources, Labe, RM, Otene, AS, Swende, LT, Njor, ST and Popoola, OB; Original Draft Preparation, Labe, RM.; Review and Editing, Otene, SA, Swende, LT., Njor, ST, and Popoola, OB; Supervision, Labe RM.; Funding, Labe, RM, Otene, SA, Swende, LT, Njor, ST, and Popoola, OB.
Conflict of Interest
The authors were enthusiastically cooperative from the start of the research to its successful completion without any element of misunderstanding or exhibition of any conflict of interest.
References
- Sung, H., Ferlay, J., Siegel, R. L., Laversanne, M., Soerjomataram, I., Jemal, A., & Bray, F. (2021). Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians, 71(3), 209-249.
- International Agency for Research on Cancer (IARC, 2022-2023). World cancer report. https://www.iarc.who.int
- World Health Organization (2022). Global cancer burden growing amidst mooning need for services. https://www.who.int
- Nigeria National Cancer Control Plan (NCCP), 2018-2022). https://www,iccp-portal.org
- Vives, L. (2022). In Nigeria, 72000 cancer death annually and rising. IDN-IndepthNews.https://indepthnews.net
- Chow, Z., Gan, T., Chen, Q., Huang, B., Schoenberg, N., Dignan, M., ... & Bhakta, A. S. (2020). Nonadherence to standard of care for locally advanced colon cancer as a contributory factor for high mortality rates in Kentucky. Journal of the American College of Surgeons, 230(4), 428-439.
- Dronkers, E. A., Mes, S. W., Wieringa, M. H., van der Schroeff, M. P., & Baatenburg de Jong, R. J. (2015). Noncompliance to guidelines in head and neck cancer treatment; associated factors for both patient and physician. BMC cancer, 15, 1-10.
- Eom, B. W., Jung, K. W., Won, Y. J., & Kim, Y. W. (2019). Trends and Outcomes of Non-compliance with Treatment for Gastric Cancer in Korea over the 16 years from 1999 to 2015. Journal of Gastric Cancer, 19(1), 92.
- Ma, A. M. T., Barone, J., Wallis, A. E., Wu, N. J., Garcia, L. B., Estabrook, A., ... & Tartter, P. I. (2008). Noncompliance with adjuvant radiation, chemotherapy, or hormonal therapy in breast cancer patients. The American journal of surgery, 196(4), 500-504.
- Borras, J. M., Font, R., Solà, J., Macia, M., Tuset, V., Arenas, M., ... & Espinàs, J. A. (2020). Impact of non-adherence to radiotherapy on 1-year survival in cancer patients in Catalonia, Spain. Radiotherapy and Oncology, 151, 200-205.
- Kleinsinger, F. (2003). Understanding noncompliant behavior: definitions and causes. The Permanente Journal, 7(4), 18.
- Hansen, LA (2024). Impact of nonadherence to cancer therapy. TON The Oncology Nurse-APNPA; https://www.theoncologynurse.com
- Stoppler, MC (2021). Definition of noncompliance. https://www.rxlist.com
- Jin, J., Sklar, G. E., Min Sen Oh, V., & Chuen Li, S. (2008). Factors affecting therapeutic compliance: A review from the patient’s perspective. Therapeutics and clinical risk management, 4(1), 269-286.
- Atinga, R. A., Yarney, L., & Gavu, N. M. (2018). Factors influencing long-term medication non-adherence among diabetes and hypertensive patients in Ghana: a qualitative investigation. PloS one, 13(3), e0193995.
- Labe, R.M., Otene, S.A., & Obochi, P.E. (2019). Perception and attitude of cancer patients toward chemotherapy administration. J Palliate Care Med; 9:355. DOI: 10.4172/2165-7386.1000355
- Deji, A (2020). There are too many fraudulent NGOs in Nigeria. https://m.facebook.com/AdeyanjudDeji1979/post/there-are-too-fraudulent-ngos-in-nigeria-theres-nothing-visible-they-do-to-1131454422206352018
- BellaNaija (March10, 2020). Let’s talk about not-for-profit organization in Nigeria. https://www.bellanaija.com
- Smith, D. J. (2010). Corruption, NGOs, and development in Nigeria. Third world quarterly, 31(2), 243-258.
- Smith, D. J. (2012). AIDS NGOS and corruption in Nigeria. Health & place, 18(3), 475-480.
- Osewa, O (March 22, 2024). Nigerian NGOs are thieves! -politics-Nigeria. https://www.nairaland.com/42142/nigeria-ngos-thieves
- Jedy-Agba, E., Curado, M. P., Ogunbiyi, O., Oga, E., Fabowale, T., Igbinoba, F., ... & Adebamowo, C. A. (2012). Cancer incidence in Nigeria: a report from population-based cancer registries. Cancer epidemiology, 36(5), e271-e278.
- Cohen, L. (2023). More people than ever are surviving from cancer in the US; study shows as research and treatment see unprecedented progress. https://www.cbsnews.com
- Uchendu, O. J. (2020). Cancer incidence in Nigeria: a tertiary hospital experience. Asian Pacific Journal of Cancer Care, 5(1), 27-32.
- American Centre for Disease Control and Prevention (n.d). Kinds of cancers. Https://www.cdc.gov
- Cancer Research UK (9 Oct, 2023). Types of cancers. https://www.cancerresearchuk.org
- Chambuso, R. S., Shadrack, S., Lidenge, S. J., Mwakibete, N., & Medeiros, R. M. (2017). Influence of HIV/AIDS on cervical cancer: a retrospective study from Tanzania. Journal of global oncology, 3(1), 72-78.
- Carter, M (2020). Women with HIV have sixfold invrease in risk of cervical cancer. https://www.hpvworld.com
- Martin, LJ & & Sreenivas, S (2022). HIV and cervical cancer: what is the link? https://www.wedmed.com
- Stelzle, D., Tanaka, L. F., Lee, K. K., Khalil, A. I., Baussano, I., Shah, A. S., ... & Dalal, S. (2021). Estimates of the global burden of cervical cancer associated with HIV. The lancet global health, 9(2), e161-e169.
- Ononogbu, U., Almujtaba, M., Modibbo, F., Lawal, I., Offiong, R., Olaniyan, O., ... & Adebamowo, C. (2013). Cervical cancer risk factors among HIV-infected Nigerian women. BMC public health, 13, 1-10.
- World Health Organization (2020). WHO release new estimates of global burden of cervical associated with HIV. https://www.who.int
- Coker. T. (n.d). cancer in Nigeria: A call to action. https://www.tchealth.com
- Folorunso, S. A., Abiodun, O. O., Abdus-Salam, A. A., & Wuraola, F. O. (2023). Evaluation of side effects and compliance to chemotherapy in breast cancer patients at a Nigerian tertiary hospital. ecancermedicalscience, 17.
- Ingwu, J. A., Idoko, C., Israel, C. E., Maduakolam, I., & Madu, O. (2019). Factors influencing non–adherence to chemotherapy: Perspective of Nigerian breast cancer survivors. Nursing Practice Today.
- Naghavi, S., Mehrolhassani, M. H., Nakhaee, N., & Yazdi-Feyzabadi, V. (2019). Effective factors in non-compliance with therapeutic orders of specialists in outpatient clinics in Iran: a qualitative study. BMC health services research, 19, 1-16.
- Singh, K., Singh, E., Rana, M. K., Sharma, P., & Sachdeva, S. (2022). Adherence to radiotherapy in the treatment of cancer patients: a tertiary care institute experience at Punjab. Asian Pacific Journal of Cancer Care, 7(1), 3-8.
- Ohri, N & Garg, M (2016). Missed radiation therapy sessions increase risk of cancer recurrence. National Cancer Institute; https://www.cancer,gov
- Palwe, V., Patil, R., Pandit, P., & Nagarkar, R. (2020). Factors influencing non-adherence to radiotherapy: a retrospective audit of 1,548 patients from a tertiary cancer centre. Journal of Radiotherapy in Practice, 19(4), 359-364.
- Umoke, I. C., & Garba, E. S. (2019). Breast cancer in North-Central Nigeria: challenges to good management outcome. International Surgery Journal, 6(9), 3105-3110.
- Vermeire, E., Hearnshaw, H., Van Royen, P., & Denekens, J. (2001). Patient adherence to treatment: three decades of research. A comprehensive review. Journal of clinical pharmacy and therapeutics, 26(5), 331-342.
- Joseph, K., Vrouwe, S., Kamruzzaman, A., Balbaid, A., Fenton, D., Berendt, R., ... & Tai, P. (2012). Outcome analysis of breast cancer patients who declined evidence-based treatment. World journal of surgical oncology, 10, 1-5.
- World Health Organization (2018). Cancer. https:/www.who.int


