Current Issue : Article / Volume 3, Issue 1
- Research Article | DOI:
- https://doi.org/10.58489/2836-5062/019
Late Cancer Presentation and Increase Palliative Care Burden on Healthcare Delivery in Makurdi Benue State: A Need for Strategic Intervention
1Department of Surgery, Federal Medical Centre Makurdi, Benue State, Nigeria
2Department of Radiology, Federal University of Health Science Otukpo, Benue State-Nigeria
3Department of Oncology and Palliative Care, Federal Medical Centre Makurdi, Benue State, Nigeria
4Department of Family Medicine, Federal Medical Centre Makurdi, Benue State, Nigeria
5Faculty of Allied Health Sciences, Baze University Abuja, Nigeria
6Oncology Department Federal Medical Centre, Abuja, Nigeria
7Department of Epidemiology and Community Medicine, College of Health Sciences, Benue State University Makurdi, Benue State, Nigeria
8Branas Isaf. Care Tech Group, United Kingdom
9Department of Internal Medicine, Benue State University Teaching Hospital Makurdi, Benue State, Nigeria
Ransome Msughve Labe*
Peteru Suega Inunduh et al (2024). Late Cancer Presentation and Increase Palliative Care Burden on Healthcare Delivery in Makurdi Benue State: A Need for Strategic Intervention. Journal of Clinical Oncology Reports. 3(1); DOI: 10.58489/2836-5062/019
© 2024 Peteru Suega Inunduh, this is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- Received Date: 20-08-2024
- Accepted Date: 29-08-2024
- Published Date: 14-09-2024
Patients, Late cancer Presentation, Palliative care burden, Healthcare delivery, Strategic Intervention.
Abstract
The study employed a narrative review design for the purpose of identifying statistical findings on late-stage cancer diagnosis from previously published studies to use as evidence to describe the prevailing incidence of patientsâ presenting with late-stage cancer disease in Benue State. The data were searched from journals indexed in Google scholar, Semantic scholar, ResearchGate, Cross-references, PubMed, DOAJ, and Abstract journals. The statistical results obtained from the review shows that, late-stage cancer presentation among people who develop the disease is a common situation in Nigeria. Specifically, to Benue State one among the few published studies reported that patients who had presented with advanced clinical diseases as evidenced by fungating masses, palpable axillary nodes, are indications of histologically established metastatic disease. Another study applying the FIGO Staging method revealed that (81.8%) presented with advanced stage disease ranging from stage IIbâIV and stage III disease was the commonest with (42.9%) of cases. A recent study revealed that (46.7%) of patients were diagnosed with stage II disease. Whereas (49.1%) presented with advanced stage III and (1.3%) stage IV disease respectively. Based on these evidences, is the pertinent need to solicit for a strategic intervention by various stakeholders in the health system to establish a specialized palliative care service facility in Benue State. Late cancer presentation is an eligible condition for palliative care; early and routine referral of cancer patients for palliative care will accord patients the benefits of enjoying improved QOL and delay of early death from the disease.
Introduction
Cancer is described as a large group of diseases that can start in almost any organ or tissue of the body when abnormal cells grow uncontrollably and migrate beyond their usual boundaries to invade adjoining parts of the body or spread to other organs [1]. The process of metastasis is evidently the major cause of death from cancer [1]. Cancer is unprecedentedly rising uncontrollably the world over. This disease is found to be the second leading cause of death and unfortunately the burden of the incidence of cancer disease has caused global concern. Sung et al (2021) [2] study showed that there are 19.3 million of cancer cases around the world. Besides, WHO reported the findings from the International Agency for Research on Cancer (IARC, 2022) survey of 115 countries an estimate of 20million cancer cases and 9.7million deaths from the disease.
In Africa, Moeti (2023) [4] in his speech on the world cancer day revealed an occurrence of approximately one million new cancer cases and 700,000 deaths occurrence. Narrowing to the sub-Saharan African States, about 626,400 and 447,000 new cancer cases and death respectively were estimated in 2012 [5, 6, 7]. The Cancer Atlas (2018) reported an estimated figure of 752,000 new cases of cancer representing 4% of the global total and 506,000 deaths occurrence. In 2020, a total of 801,392 new cases and 520,158 deaths was reported [9]. Another statistical report showed a total of 848,311 new cases of cancer and 559,083 deaths [10]. There is an obvious concern that the rising cases of cancer in the Sub-Saharan Africa, and other developing countries, Nigeria inclusive will by the year 2030 account for approximately 70% of all new cases of cancer [7]. Invariably, the conspicuous soaring rate of the disease has affirmed the assertion that cancer is a major public health problem in sub-Saharan Africa, affecting many of the region’s 1 billion inhabitants [9].
By independent country, quantum of evidence from available studies showed that the prevalence of cancer in Nigeria is epidemiologically on the rise. For example, the incidence of cancer is estimated at 102,000 of new cases and 72,000 deaths in annually in Nigeria[11]. A grimly growing figure of 95,950 and 60,471 for new cases of cancer and deaths is from fifteen types of cancer-like gallbladder, melanoma of skin, oesophagus, bladder, kaposi sarcoma, lung, Hodgkin lymphoma, kidney, colon, leukaemia, liver, non-Hodgkin lymphoma, cervix uteri, prostate and breast cancers [7]. A study reviewed the incidence and mortality rate of cancer in Nigeria from a Population-based Cancer Registries estimated the incidence rate for all invasive cancers from the IBCR of 66.4 per 100 000 men and 130.6 per 100,000 women. In ABCR it was 58.3 per 100 000 for men and 138.6 per 100 000 for women [12]. The findings from a recent study of 430 cancer patients referred for chemotherapy in Oncology and Palliative Care Clinic Federal Medical Centre Makurdi, Benue State showed that fifty-three different types of cancers were diagnosed in males and female patients. The most frequent were breast cancer 115(26.7%), cervical cancer 89(20.7%), liver cancer 19(4.4%), ovarian cancer, 16(3.7%), colorectal cancer 15(3.5%), non-Hodgkin lymphoma 15(3.5%), and nasopharyngeal cancer 11(2.6%). [13]
Late-Stage Cancer Presentation
Besides the disturbing rise in the cases of cancer in Benue State and Nigeria as whole, patient’s late-stage cancer presentation is seemingly endemic. Late or delayed cancer presentation as it is used interchangeably, refers to a situation whereby a patient did not seek for medical treatment to identified symptoms of the cancer disease earlier as would be expected until it is confirmed medically that it has metastasized to other parts of the body. The national cancer institute describes late cancer presentation as a term used to describe cancer that is far along in its growth, and has spread to the lymph nodes or other places in the body. According to some researchers, late or delayed cancer presentation refers to a patient who presents with appearance of symptoms of the disease that is more than two to three months in a healthcare facility for consultation with medical doctor [14, 15].
The Unfortunate problem of late cancer presentation is in the fact that, majority of cancer patients in Nigeria are diagnosed of a cancer that has characteristics of advanced stage disease irrespective of the cancer type. Numerous studies have been found significant evidences related to this reality. For examples, 17.7% of patients diagnosed with breast cancer presented with stage III and IV disease respectively [7]. A study of 105 cervical patients found that 72-81% of patients presented with a late-stage disease [16]. 68.8% out of 61 breast cancer patients in Port Harcourt presented with late-stage disease [17]. 3% late presentation with malignant tumour, 49.8 Percent and 28.6 Percent cancer patients treated with radiotherapy presented with stage I, III and IV in Sokoto State [18]. 55.3% of breast cancer patients in Southwest Nigeria presented at stage III and IV 3.9% [19]. 92% of cancer patients studied from a tertiary hospital in Niger-Delta were found with delayed disease presentation [20]. Thus, as mentioned earlier, the perception is that the prevailing cases of late-stage cancer presentations in Nigeria would likely get worse by the year 2030 [21].
Apparently, late presentation of cancer is recognized to lead to negative treatment outcome, poor clinical prognosis, increased risks of side effects from the use of second-or-third-line treatment, incurred high cost of treatment, impaired competence to function and reduced chances of the patient survival.[22, 23, 24], Deducing from the numerous empirical evidences on late cancer presentation situation in Nigeria, it will be reasonable to conclude that, medical interventions with all necessary treatment procedure for patients diagnosed with cancer have been majorly palliative care. Palliative care is a medical care intervention that is planned primarily to be a patient-and-family centred intervention through a multidisciplinary approach for assessment, diagnosis and treatment of people living with life-threatening illness such as cancer [25].
The foremost objective of palliative care is to relief symptoms of pain (physical and emotional) and any other distress related with physical, psychosocial, and spiritual issues that could be potentially impairing the individual functioning and quality of life [21]. Palliative care is a medico-psychosocial intervention that is necessary and essential to cancer patients whose disease condition has grown beyond the probable expected cure. Palliative care services help to minimize the outrageous signs and symptoms of advanced stage disease that castrate patients emotional and physical wellbeing and general health deterioration that propels patients to early entrance in the hydra mouth of impending death. Patients who are exposed to effective palliative care intervention are at the advantage of experiencing improve quality of life and some reasonable extended years of living.
Apparently, there are numerous studies that have published valid empirical findings on the burden of cancer disease emerging from higher prevalence rate leading to an unabating mortality rate of people who are with the disease. Beyond the problem of growing rate of cases, another disturbing situation recognized in the population of cancer patients in Benue State is; patients seeking treatment are found to be commonly presenting with features of advanced stage cancer disease that is worsening with noncompliance to standard treatment procedures even when treatment commences [13, 14, 26]. Invariably, these prevailing situations have greater harmful potential to expose the cancer patients to rapid disease progression, aggravated excruciating pains and experience of greater waves of emotional disturbance that persist to the end-of life. Extrapolating from these concerns, the study seeks to reveal the magnitude of patients’ late-stage cancer presentation that is increasing cancer care burden on the already overstretched public healthcare system in Benue State and the need have a specialize palliative care facility.
Aim/Objectives
The primary purpose of the study was based on identifying and gathering preferred and needed quantity of empirical data from previous published studies on late-stage cancer presentation by patients in the hospitals in order to describe and explain its impact on increase burden of palliative care in Benue State. The objectives are to:
- Describe the existing reality of the prevailing situation of patients presenting with late-stage cancer disease in the hospitals in Benue State.
- Establish that diagnosis of patients’ late-stage cancer presentation instead of early presentation for radical intervention is rapidly growing into palliative care burden.
- Draw the attention of the government and other relevant stakeholders to the situation as well as demand for the need to establish of a palliative care service centre in Benue State.
Research Questions
- To what extent do people who develop cancer present with a late-stage disease in Benue State?
- How does late-stage cancer presentation result into a palliative care burden in Benue State?
- What are the benefits of the need for establishment of a palliative care service centre in Benue State?
Methods
Research Design
The study employed a narrative review research design to provide an insightful understanding of the burden of cancer and late stage presentation of the disease by patients, which is unfortunately limiting their chances of survival or prolong living. Narrative review research provides a flexible and rigorous method to conduct a rich study by doing a meaningful survey of related existing literature that can be used as evidence to support the researcher’s position on the topic of problem of interest [27]. The focus of the study is to bring to limelight the undesirable burden of patients’ late-stage cancer presentation for diagnosis which is recognized as a palliative care problem in cancer management.
Data Collection
The data for the study were precisely empirical results from previous published researches in Nigeria and Benue State on late-stage cancer presentation. Thus, with the narrative review technique of sampling of the relevant literature, the search to obtain the data was done in the open access peer reviewed journals articles published and archived in various internet database and meta-bases. Much of these statistically required data were lifted from journals indexed in Google scholar, Semantic scholar, ResearchGate, Cross-references, PubMed, DOAJ, and Abstract journals.
Results
The study results are from the identified relevant previously published studies presented for discussion to fulfil the aim of the perceived problem of interest. Actually, due to the paucity of researches on cancer incidence in Benue State, only three studies were found available to rely on as evidences.
Table 1: Summary of breast cancer presentation features of advanced stage disease
| Features | Frequency | Percentage (%) |
| Palpable axillary nodes | 59 | 56.7 |
| Fungating masses | 99 | 59 |
| Associated ulceration | 24 | 26 |
Source: Echejoh et al (2011) [28]
Table one described the identified features of late-stage cancer presentation of 315 breast cancer patients from archival record of all breast biopsies from January, 1997 to December, 2006 in the histopathology department of Federal Medical Centre, Makurdi in Benue State [28].
Table 2: Distribution of histological type and stage of cancer
| Variables | Frequency (N=77) | Percentage (%) |
| Type of cancer | ||
| Squamous cell carcinoma | 72 | 97.4 |
| Adenocarcinoma | 2 | 2.6 |
| Stage of cancer | ||
| I–II | 14 | 18 |
| IIb | 13 | 16.9 |
| III | 33 | 42.9 |
| IV | 17 | 22.1 |
Source: Hembah-Hilekaan and Anenga (2024) [29]
Table two shows the researchers application of the FIGO Staging method which revealed that 63(81.8%) presented with the advanced stage of the disease stage IIb–IV. Only 14(18.2%) presented with early-stage cancer of (I–IIa). In all, stage III disease was the commonest with 33(42.9%) of cases [29].
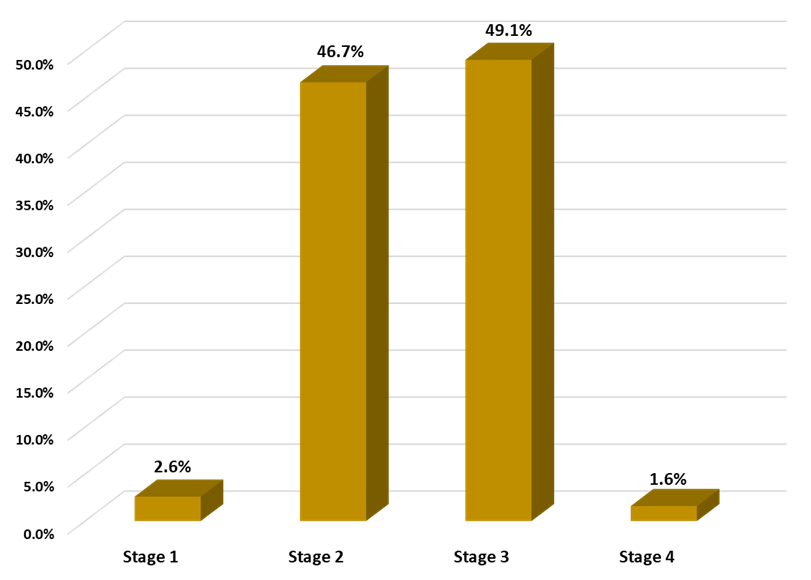
Fig 1: Bar chart distribution of late-stage cancer presentation by patients.
Source: Otene, Labe. Swende, Injor and Popoola (2024) [13]
The bar charts described the statistical evidence of histological diagnosis of late-stage cancer presentation by patients which has been documented in the patients’ folders accessed in the record unit of the Oncology and Palliative Care department in Federal Medical Centre Makurdi. On the bar chart, 46.7% of patients were diagnosed with stage II disease, 49.1 percent advanced stage III and 1.3% stage IV disease [13].
Discussion
Actually, there is generally a paucity of research to provide adequate data to explain the magnitude of the incidence of cancer in Benue State for many reasons. However, there is a prevailing noticeable disturbing situation of late-stage cancer presentation by patients who has developed the disease as commonly seen from their histological results obtained from biopsies. The prevailing cases of late cancer presentation in the already growing population of cancer patients in Benue State is clearly shifting into a palliative care burden. Research wise, as earlier mentioned, there are not enough studies to use as substantial evidences to demonstrate the influence of late-stage cancer presentation on increasing palliative burden on already overstrained healthcare system in Benue State. Thus, discussion used statistical results of only three published cancer related researches late-stage cancer presentation, increase palliative care burden and the need for government to establish a palliative centre in Benue State. The discussion focuses on answering the three stated research questions.
Question 1: To what extent do people who develop cancer present with a late-stage disease in Benue State?
The increasing prevalence of the development of cancer disease in the Nigeria population nowadays is unwholesomely swelling the existing public health challenges. It has come to be that every day, two to three people are diagnosed with one type of cancer disease or the other in adult males, females and children respectively. This is only known from those who enter the hospitals to seek medical treatment of observed unusual persisting signs and symptoms of malady in a particular part of the body. They are actually many other people who have not gone to the hospital despite experiencing this unusual illness that might be characteristically a cancer. But they are consulting with the traditional medicine practitioners in their communities for its treatment. This makes it difficult to have accurate statistical data to announce exactly the rate at which cancer is rapidly increasing in Benue State.
However, based on the official hospital records, researchers’ published findings and the frequency with which people are diagnosed with cancer; these daily oncoming number of patients shows there is an unprecedented soaring case of cancers in Benue States. Beside the rapid growing incidence of cancer cases is the disturbing clinical observation from the histological results of cancer biopsies that, constantly patients are diagnosed with late-stage cancers. Late-stage cancer presentation is conspicuously becoming an undesirable national health problem. And this by extension, it is influencing the growing mortality rate of the country’s population. There are many studies across all states in the six geopolitical zones that have published empirical evidence about this situation in Nigeria [11, 15, 16, 17, 18, 19, 20].
To be specific on Benue State, the extent of the frequent clinical evidence of patients diagnosed with features of late-stage cancer from biopsies have been revealed from fewer studies. For example, Echojoh et al [2011] examination of archival records of 1418 tissue biopsies from January, 1997 to December, 2006 found that 59 (56.7%), 99(59%), and 24(23%) of 315 breast biopsies had positive axillary nodes, palpable masses, and associated ulceration that showed features of late cancer presentation. At the Benue State University Teaching Hospital 63(81.8%) presented with the advanced stage disease of stage IIb–IV. Only 14(18.2%) presented with early cancers of stage I–IIa. Stage III disease was the commonest with 33(42.9%) cases [29]. In Federal Medical Centre Makurdi, 46.7% of patients were diagnosed with stage II disease, 49.1 percent advanced stage III and 1.3% stage IV of various cancers. Breast and cervical cancer patients are mostly associated with late-stage presentation of the disease [13].
Question 2: How does late-stage cancer presentation result into a palliative care burden in Benue State?
Medical practitioners in oncological intervention has acknowledge that only five to seven cancers can be 100% completely cured and they include breast (early stage), prostate cancer, melanoma, thyroid, Hodgkin lymphoma, cervical and testicular cancers. Even so, some experts contended that there is no complete guarantee that a person will be cured of cancer as there is the probability of reoccurrence [30 31, 32]. As a result, oncologists prefer to use the term remission when it comes to cancer recovery. This implies that for cancer treatment of ones that can be cured and many others that cannot be cured, palliative care is inevitably required at the starting point [31, 32]. This is likely because at the very point of diagnosis even though the tumour may be localized and not actually threatening. But the patient’s psychological, social and spiritual equilibria and tranquil state instantly become dislocated. In view of this, evidence have shown that access to early integrated PC is essential approach for the management of patients to improve their QOL and survival [33]. It also means that PC can be provided from the onset of diagnosis to end-of-life care.
Definitely, not all patients would need palliative care, but it is essential that they should have access to it for optimum mitigation of physical and psychological symptoms control [34, 35]. In addition, other evidence-based studies recommended early PC involvement especially for patients with uncontrolled symptoms and QOL concern [36]. Palliative care is associated with survival benefits among patients with advanced stage cancer [37]. These and many other evidence-based studies have substantially justified that the unabating situation of patients’ late-stage cancer presentation in Benue State is an indication of increase in palliative burden on the limited resources of the healthcare facilities. This unquestionably is a pointer to the need for the government and other stakeholders’ strategic intervention to establish a specialize palliative facility. This will help in the better management of cancer patients eligible for palliative care as well decongest the pressure on the only already overstretched two tertiary hospitals that are treating cancer Benue State.
Question 3: What are the benefits of the need for establishment of a palliative care service centre in Benue State?
Palliative care looks at how the cancer experience is affecting the whole person by helping to relieve symptoms, pain, and stress. It gives patients options and allows them and their caregivers to take part in planning their care. It’s about making sure that all their care needs are addressed [31]. PC benefits the patients by helping to minimize the awful signs and symptoms of advanced stage disease that castrate patients emotional and physical wellbeing leading to general health deterioration that accelerate his or her early entrance in the planet of death. Cancer patients who are exposed to effective palliative care intervention are at the advantage of experiencing improve quality of life and some reasonable extended years of living. In Sanders et al (2024) report, many studies have shown that referral of patients with advanced cancer early to specialized palliative care leads to improved QOL.
PC helps the patient and their family along the treatment journey decrease pain, depression, stress and worry. It can also help families who are struggling with a loved ones’ disease to obtain relief from the distress of caregiving where it is only them are left with the patient. It is also reported that patients who received early palliative care scores better on an assessment of their ability to cope with their disease and are more likely to discuss end-of-life care preferences with their healthcare team. Therefore, frequent palliative care referrals may be more advisable at diagnosis in poor prognosis cancers. This means that late-stage cancer diagnosis are unequivocally eligible patients for PC and it is pertinent that they should be routinely referred to access palliative care services in order they will gain its aforementioned benefits satisfactory to the end-of life.
Conclusion
Cancer has become a common disease people are developing nowadays not only in Benue State alone but also in Nigeria as a whole. Sadly, to this is the irrefutable reality that the frequency of late stage cancer diagnosis in the patients is conspicuously alarming nationwide. Many studies reviewed in this current research have published validly empirical findings to describe the reality of this observed situation of patient’s late cancer presentation on seeking medical treatment. The bad effect of this is the additional burden it is imposing on the limited resources healthcare system in the country generally. By virtue of this concern, there is the need to draw the attention of the government and other stakeholders to the importance of intervention by establishing palliative care service centre in Benue State. Palliative care is a specialized medical treatment approach and is recommended as a standard part of care given to people with cancer. Palliative care is appropriate for people of any age and at any stage in any serious illness.
Recommendations
Apart from the call on the government for intervention to establish a palliative care centre in Benue State, it is relevant for medical health professionals and the ministry of health to work in collaboration for the followings.
- The government and other stakeholders in the healthcare system should extend their strategic investment policy and concepts to establish a palliative care centre in Benue State to mitigate the increasing burden of cancer care on the only two tertiary health institutions which are already overstretched and are functioning below the standard requirements to achieve international best practices.
- It is pertinent to appeal and encourage the ministry of health in Benue State to collaborate with the medical health professionals to initiate and embark on effective community-based campaign focused on educating and enlightening the citizens on the importance of early seeking of medical intervention on a perceived persisting unusual signs and symptoms of ill-health for early diagnosis and treatment.
- The government as well as the management of the healthcare institutions in Benue State should endeavor to adopt a proactive and sustainable policy to train their healthcare workers in palliative care, which is a specialized medical treatment recommended as a standard part of care given to people with cancer.
- Palliative care training programme and/or courses should be included in the curriculum of the various health institutions of learning in the Benue State in order that it will offer opportunities to people to seek and gain admission to study or be trained in palliative care.
Acknowledgement
We like to appreciate all the authors for their commitment and roles to ensure that we had quality research out of the conceived topic to bring to limelight the issue of patients’ late-stage cancer presentation and to draw the government and other stakeholders’ attention to the need to establish a palliative centre in Benue State. We specially thank Dr Ransome Msughve Labe for the effective coordination of the research with relentless motivation of the coauthors.
Funding
The authors sponsored the study from their out-of-pocket contributions.
Authors Contributions
The contributions of the authors were in the following ways; Research Idea and Topic: Dr PS Inunduh and Dr RM Labe; Data Search: Dr RM Labe; Original Draft Preparation, Dr RM Labe; Review and Editing: Dr PS Inunduh, Dr AS Otene, Dr AD Daniel, LT Swende; Coordinator and Supervision: Dr RM Labe and Dr PS Inunduh; Funding: Dr PS Inunduh, Dr RM Labe, AS Otene, Dr LT Swende, Dr AD Daniel, ST Injor, Dr OB Popoola, OB Ornguga, NA Akwaras, TO Ahmadu, GN, Rimamnunra and DO Ayatse.
Conflict of Interest
The authors were cooperative to the end of the study without expression of any conflict of conflict.
References
- Mattiuzzi, C., & Lippi, G. (2020). Cancer statistics: a comparison between world health organization (WHO) and global burden of disease (GBD). European journal of public health, 30(5), 1026-1027.
- Sung, H., Ferlay, J., Siegel, R. L., Laversanne, M., Soerjomataram, I., Jemal, A., & Bray, F. (2021). Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians, 71(3), 209-249.
- Cao, W., Qin, K., Li, F., & Chen, W. (2024). Comparative study of cancer profiles between 2020 and 2022 using global cancer statistics (GLOBOCAN). Journal of the National Cancer Center.
- Müller, S. A., Elimian, K., Rafamatanantsoa, J. F., Reichert, F., Mosala, F., Böff, L., ... & El-Bcheraoui, C. (2024). The burden and treatment of non-communicable diseases among healthcare workers in sub-Saharan Africa: a multi-country cross-sectional study. Frontiers in Public Health, 12, 1375221.
- Uchendu, O. J. (2020). Cancer incidence in Nigeria: a tertiary hospital experience. Asian Pacific Journal of Cancer Care, 5(1), 27-32.
- Howlader, N. N. A. K. M., Noone, A. M., Krapcho, M., Garshell, J., Miller, D., Altekruse, S. F., ... & Cronin, K. A. (2014). SEER cancer statistics review, 1975–2012. National Cancer Institute.
- Rabiu, I., Isah., J.A., & Muhammad, A. (2023). Insights into the rising cases of cancer in Nigeria. Int J cell Sci & mol biol; Volume 7. Issue 3. DOI: 10.19080/IJCSMB.2023.07.555712
- The Cancer Atlas (2018). Sub-Saharan Africa ǀ The Cancer Atlas. https://canceratlas.cancer.org
- Bray, F., Parkin, D. M., Gnangnon, F., Tshisimogo, G., Peko, J. F., Adoubi, I., ... & Chingonzoh, T. (2022). Cancer in sub-Saharan Africa in 2020: a review of current estimates of the national burden, data gaps, and future needs. The Lancet Oncology, 23(6), 719-728.
- Global Cancer Observatory (GLOBOCAN, 2022). Sun-Saharan African. https://gco.iarc.who.int
- Otene, S. A., Labe, R. M., Swende, L. T., Njor, S. T., & Popoola, O. B. (2024). Noncompliance to Standard Treatment Procedures for Cancer Propelling Increase in the Mortality Rate of Cancer Patients in Benue State, Nigeria. Cancer Research and Cell Development, 3(1).
- Jedy-Agba, E., Curado, M. P., Ogunbiyi, O., Oga, E., Fabowale, T., Igbinoba, F., ... & Adebamowo, C. A. (2012). Cancer incidence in Nigeria: a report from population-based cancer registries. Cancer epidemiology, 36(5), e271-e278.
- Otene, S.A., Labe, R.M., Swende, L.T. Injor, S.T. & Popoola, O.B. (2024). Noncompliance to standard treatment procedures propelling increase in the mortality rate of cancer patients in Benue State, Nigeria. Cancer Research and Development.; 3(1)
- Khan, M. A., Hanif, S., Iqbal, S., Shahzad, M. F., Shafique, S., & Khan, M. T. (2015). Presentation delay in breast cancer patients and its association with sociodemographic factors in North Pakistan. Chinese Journal of Cancer Research, 27(3), 288.
- Bhuiyan, M. M. Z. U., Maele, M. M., Mavhungu, R., & Ooko, F. (2022). Breast cancer: Factors influencing late-stage presentation at the Mankweng Hospital breast cancer clinic, Polokwane, Limpopo Province, South Africa. South African Medical Journal, 112(11), 906-910.
- Awofeso, O., Roberts, A. A., Salako, O., Balogun, L., & Okediji, P. (2018). Prevalence and pattern of late-stage presentation in women with breast and cervical cancers in Lagos University Teaching Hospital, Nigeria. Nigerian Medical Journal, 59(6), 74-79.
- Elenwo, S. N., Ijah, R. F. O. A., & Dimoko, A. A. (2022). Factors associated with late presentation of breast cancer in a Teaching Hospital in Port Harcourt, Nigeria. Nigerian Health Journal, 22(1), 140-152.
- Aliyu, U. M., Jimoh, A. O., & Yunusa, A. (2015). Pattern of cancers treated with radiotherapy in Uduth Sokoto: a new center experience. Journal of Clinical and Diagnostic Research: JCDR, 9(8), XC01.
- Ali-Gombe, M., Mustapha, M. I., Folasire, A., Ntekim, A., & Campbell, O. B. (2021). Pattern of survival of breast cancer patients in a tertiary hospital in South West Nigeria. ecancermedicalscience, 15.
- Agbonrofo, P. I., & Eriba, L. O. (2020). Audit of delayed presentation in breast cancer from a tertiary centre in the Niger Delta, Nigeria. Ibom Medical Journal, 13(3), 164-171.
- Ayetoto-Oladeinde, T. (2023). Nigeria’s late-stage cancer crisis could worsen by 2030. March 27,
- Cross, C., Mokua, S., Ngilangwa, R., Santos, C., Ngoma, T., & Mujinja, P. G. (2024). Beyond “Late Presentation”: Explaining Delayed Cancer Diagnosis in East Africa. In Cancer Care in Pandemic Times: Building Inclusive Local Health Security in Africa and India (pp. 93-111). Cham: Springer International Publishing.
- Damsees, R., Jaghbir, M., Salam, M., Al-Omari, A., & Al-Rawashdeh, N. (2023). Unravelling the predictors of late cancer presentation and diagnosis in Jordan: A cross-sectional study of patients with lung and colorectal cancers. BMJ open, 13(5), e069529.
- Singletary, S. E., Allred, C., Ashley, P., Bassett, L. W., Berry, D., Bland, K. I., ... & Greene, F. L. (2002). Revision of the American Joint Committee on Cancer staging system for breast cancer. Journal of clinical oncology, 20(17), 3628-3636.
- Dolan, R. D., Maclay, J. D., Abbass, T., Colville, D., Buali, F., MacLeod, N., ... & McMillan, D. C. (2020). The relationship between 18F-FDG-PETCT-derived tumour metabolic activity, nutritional risk, body composition, systemic inflammation and survival in patients with lung cancer. Scientific Reports, 10(1), 20819.
- World Health Organization. (2021). Assessing the development of palliative care worldwide: a set of actionable indicators.
- Sukhera, J. (2022). Narrative reviews in medical education: key steps for researchers. Journal of Graduate Medical Education, 14(4), 418-419.
- Echejo, G.O., Dzuachii, D.O., & Jenrola, A.A. (2011). Histopathological analysis of breast cancer in Makurdi, Northcentral Nigeria. journal of Medicine in the Tropics; Vol.3, No 1. Doi: 10.4314/jmts.v/3i/.69328
- Hembah-Hilekaan, S. K. (2022). A Seven-Year Review of Cervical Cancer in a Tertiary Hospital in Makurdi, Nigeria. Tropical Journal of Obstetrics and Gynaecology, 39(2), 18-24.
- Thomas, T.H. (2023). What are the most curable cancers? MedicalNewsToday.
- Madomo, C. (2024). What are the most curable cancers? Health.
- Robinson, J. (2024). 5 curable cancers.
- Janah, A., Gauthier, L. R., Morin, L., Bousquet, P. J., Le Bihan, C., Tuppin, P., ... & Bendiane, M. K. (2019). Access to palliative care for cancer patients between diagnosis and death: a national cohort study. Clinical epidemiology, 443-455.
- American Cancer Society (2019). Palliative care. cancer.org | 1.800.227.2345;
- Islam, J. Y., Nogueira, L., Suneja, G., Coghill, A., & Akinyemiju, T. (2022). Palliative care use among people living with HIV and cancer: an analysis of the National Cancer Database (2004-2018). JCO Oncology Practice, 18(10), e1683-e1693.
- Sanders, J. J., Temin, S., Ghoshal, A., Alesi, E. R., Ali, Z. V., Chauhan, C., ... & Ferrell, B. R. (2024). Palliative care for patients with cancer: ASCO guideline update. Journal of Clinical Oncology, JCO-24.
- Sullivan, D. R., Chan, B., Lapidus, J. A., Ganzini, L., Hansen, L., Carney, P. A., ... & Slatore, C. G. (2019). Association of early palliative care use with survival and place of death among patients with advanced lung cancer receiving care in the Veterans Health Administration. JAMA oncology, 5(12), 1702-1709.


