Article In Press : Article / Volume 3, Issue 1
- Case Report | DOI:
- https://doi.org/10.58489/2836-502X/012
Primary Squamous Cell Carcinoma of Thyroid: A Rare Case Report.
1A.J. Institute of Medical Sciences, Kuntikana, Mangalore 575 003, Karnataka, India,
2Resident, Department of General Surgery, A.J. Institute of Medical Sciences & Research centre, Mangalore,
3Vishwanath, Department of Surgical Oncology, A J Hospital & Research Centre, Mangalore, India.
4Professor and Chair, Department of Pathology, A.J. Institute of Medical Sciences & Research centre, Mangalore.
Anand Bhandary Panambur *
Anand Bhandary Panambur, K Rahul Shenoy, Vishwanath, Thoppil Reba Philipose, (2024). Primary Squamous Cell Carcinoma of Thyroid: A Rare Case Report. Endocrine System and Diabetes. 3(1); DOI: 10.58489/2836-502X/012
© 2024 Anand Bhandary Panambur, this is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- Received Date: 07-08-2024
- Accepted Date: 22-08-2024
- Published Date: 06-09-2024
Thyroid carcinoma, Primary Squamous cell carcinoma of thyroid gland, total thyroidectomy and central neck dissection, dedifferentiation.
Abstract
Primary squamous cell carcinoma (PSCC) of the thyroid gland is a rare pathology because there is no squamous epithelium in the thyroid gland. Primary squamous cell carcinoma of the thyroid gland is rare of the thyroid malignancy, accounting for < 1% of all reported cases globally. It is extremely aggressive in nature and has a poor prognosis. We offer a case report of a female patient who presented with neck swelling â Solitary thyroid nodule of right lobe of thyroid; FNAC misinterpreted it as papillary carcinoma of the thyroid and redo FNAC using image guidance showed it to be PSCC. Patient underwent total thyroidectomy with central neck dissection and right modified radical neck dissection, and HPE revealed it to be a case of moderately differentiated squamous cell carcinoma of the thyroid. Our workup is discussed, including the distinction from metastatic illness, etiology of squamous cell carcinoma in thyroid and possible hypothesis behind dedifferentiation and metaplastic theory.
Introduction
Primary squamous cell carcinoma (PSCC) of the thyroid represents less than 1% of all primary thyroid malignancies and only a few cases have been reported in the world literature1. Before diagnosing case as a primary squamous cell carcinoma of thyroid, possibility of other primary focuses of squamous cell carcinoma which can metastasize to thyroid must be excluded. PSCC of thyroid is described as a very aggressive tumor with a poor prognosis. The median survival after diagnosing a PSCC of thyroid is less than six months. Herein, we report a rare case of primary squamous cell carcinoma of thyroid presented as a solitary thyroid nodule.
Case Report
A 58-year-old female presented with a painful tender swelling in her right lower neck for two months. She had history of rapid growth of the swelling over the last two weeks. There was no history of thyroid hyper- or hypo function. She was not addicted to smoke or alcohol. Examination revealed a hard single nodule in the right lobe of the thyroid, as well as a palpable right cervical lymph node at level IIa. Fine needle aspiration cytology (FNAC) from the thyroid nodule performed in another lab indicated papillary cancer of the thyroid, while another from the other lab revealed malignant thyroid growth. FNAC from the right thyroid lobe nodule and right cervical lymph node was performed under imaging guidance in our center, revealing primary thyroid squamous cell cancer.
A computed tomography (CT) scan of the neck revealed a soft tissue density mass originating from the right lobe of the thyroid and extending up to the suprasternal region, compressing the hypopharynx and effacement of the pyriform sinus. Laryngoscopy was normal. The patient underwent an upper GI endoscopy, which was normal. Due to financial constraints, the patient did not receive a PET CT. So we performed a total thyroidectomy Fig.01 with central neck dissection (CND) and clearance with right sided modified radical neck dissection (MRND) type I. Intraoperatively, a hard nodule emerging from the right lobe of the thyroid was discovered infiltrating thyroid cartilage, pharyngeal constrictors, and the esophagus posteriorly. Level II, III, and IV enlarged
cervical LNs were observed and encasing the right IJV, with the jugular vein being thrombosed and infiltrating the right carotid sheath.
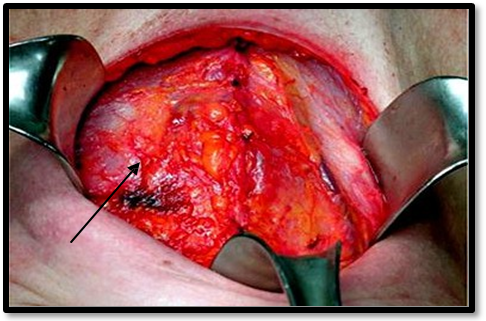
Fig.01 Showing intra-operative image of total thyroidectomy and the thyroid gland with Solitary thyroid nodule in the right lobe.
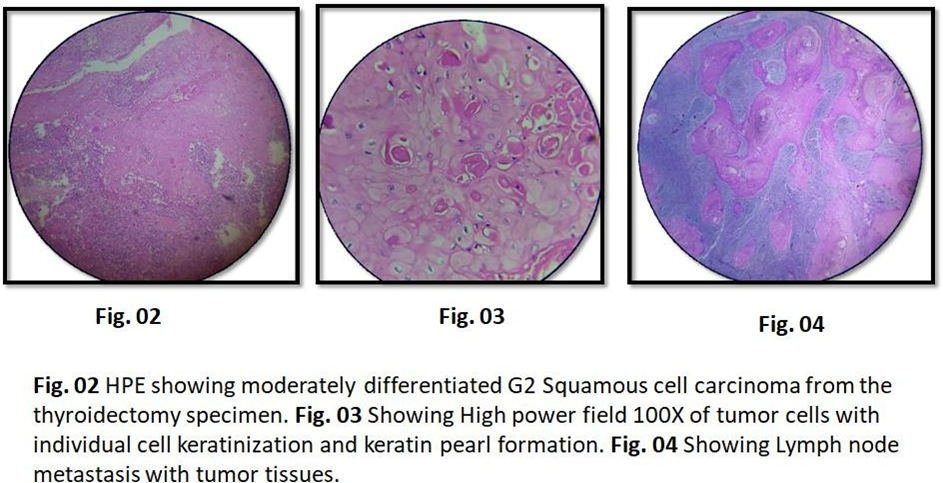
The patient tolerated the procedure well, and the early postoperative period was unremarkable. A histopathological examination (HPE) of the thyroid specimen indicated a moderately differentiated squamous cell carcinoma (S.C.C) of the thyroid Fig.02 & Fig. 03 with lymph node metastases, extra nodal extension (ENE) Fig.04, and invasion of the neighboring soft tissue. Adjuvant radiation was scheduled for the next follow-up visit, but the patient did not follow up with our institute thereafter.
Discussion
Because the thyroid gland lacks squamous epithelium, Primary SCC (PSCC) of thyroid is a rare pathology, accounting for less than 1% of thyroid carcinoma and with just a few case reports have been recorded in the literature1. It behaves like an anaplastic carcinoma, with a median survival of less than six months, frequently due to airway infiltration2. PSCC of the thyroid primarily affects female patients in their fifth or sixth decade of life, frequently with a history of goiter / solitary thyroid nodule3. As in our situation, the patient may complain of fast growth of the nodule. Often, tumors infiltrate the surrounding structures at the time of presentation, making oncological plan for management difficult.
The final diagnosis of primary squamous cell carcinoma (SCC) of the thyroid is determined by its unique microscopic morphology, the exclusion of other possible primary lesions, and the use of immunohistochemistry. 3 Differential diagnoses for primary SCC of the thyroid include anaplastic carcinoma, metastatic SCC, and carcinoma showing thymus- like differentiation (CASTLE). Differentiating between primary and secondary SCC is crucial and involves ruling out primary lesions in other organs mainly in Head and neck depending upon the concept of field cancerisation. Since the thyroid gland does not contain squamous cell epithelium, the origin of squamous cell carcinoma in the thyroid is highly debated. Several theories 6 have been proposed to explain this phenomenon, including the embryonic nest cell theory7, the metaplastic theory,8 and the dedifferentiation theory. 9
In recent years, the metaplastic theory has gained acceptance due to several case reports. Some researchers have documented primary squamous cell carcinoma (PSCC) of the thyroid occurring in the context of lymphocytic thyroiditis, suggesting that continuous stimulation leads to squamous metaplasia of follicular cells. 10 Due to its rarity, the efficacy and outcomes of chemoradiation in treating thyroid PSCC have not been extensively studied. However, numerous studies have reported poor responses to both chemotherapy and irradiation. 6, 11 Consequently, the optimal treatment strategy involves early detection and aggressive surgery aimed at achieving an R0 resection, although this is not always feasible.
Conclusion
Primary squamous cell carcinoma (PSCC) of the thyroid is a highly rare and severe cancer with a median survival of six months. PSCC of thyroid infiltrates around structures is frequently seen at presentation. It is resistant to chemotherapy and radiotherapy, and surgery with R0 resection should be the preferred treatment whenever possible. Before identifying the case as a thyroid PSCC, a complete clinical workup is required to rule out the major focus. This case should raise awareness about the disease's aggressive nature and the absence of known therapeutic alternatives. Irrespective of the rarity of this disease process, a deeper discussion of diagnostic criteria should be pursued in oncology platform and groups which will further facilitate to set certain guidelines and oncologic protocol.
Disclosures
Conflict of Interest Statement
The authors have no conflicts of interest to declare.
Funding Sources
The authors did not receive any funding.
References
- Korovin, G. S., Cho, H. T., Kuriloff, D. B., & Sobol, S. M. (1989). Squamous cell carcinoma of the thyroid: a diagnostic dilemma. Annals of Otology, Rhinology & Laryngology, 98(1), 59-65.
- Lam, K. Y., Lo, C. Y., & Liu, M. C. (2001). Primary squamous cell carcinoma of the thyroid gland: an entity with aggressive clinical behaviour and distinctive cytokeratin expression profiles. Histopathology, 39(3), 279-286.
- Sapalidis, K., Anastasiadis, I., Panteli, N., Strati, T. M., Liavas, L., Poulios, C., & Kanellos, I. (2014). Primary squamous cell carcinoma of the thyroid gland. Journal of Surgical Case Reports, 2014(12), rju133.
- Kakudo, K., Bai, Y., Ozaki, T., Homma, K. I., Ito, Y., & Miyauchi, A. (2013). Intrathyroid epithelial thymoma (ITET) and carcinoma showing thymus-like differentiation (CASTLE). CD5-positive neoplasms mimicking squamous cell carcinoma of the thyroid.
- Lui, J. T., Khalil, M. N., & Chandarana, S. P. (2014). Primary squamous cell of the thyroid–an abbreviated clinical presentation. Journal of Otolaryngology-Head & Neck Surgery, 43(1), 17.
- Syed, M. I., Stewart, M., Syed, S., Dahill, S., Adams, C., McLellan, D. R., & Clark, L. J. (2011). Squamous cell carcinoma of the thyroid gland: primary or secondary disease? The Journal of Laryngology & Otology, 125(1), 3-9.
- Goldberg, H. M., & Harvey, P. (1956). Squamous-cell cysts of the thyroid with special reference to the aetiology of squamous epithelium in the human thyroid. Journal of British Surgery, 43(182), 565-569.
- Chaudhary, R. K., Barnes, E. L., & Myers, E. N. (1994). Squamous cell carcinoma arising in Hashimoto's thyroiditis. Head & neck, 16(6), 582-585.
- Lam, A. K. Y. (2020). Squamous cell carcinoma of thyroid: a unique type of cancer in World Health Organization Classification. Endocrine-related cancer, 27(6), R177-R192.
- Lui, J. T., Khalil, M. N., & Chandarana, S. P. (2014). Primary squamous cell of the thyroid–an abbreviated clinical presentation. Journal of Otolaryngology-Head & Neck Surgery, 43(1), 17.
- Sarda, A. K., Bal, S., Arunabh, Singh, M. K., & Kapur, M. M. (1988). Squamous cell carcinoma of the thyroid. Journal of Surgical Oncology, 39(3), 175-178.
- Kebapci, N., Efe, B., Kabukcuoglu, S., Akalin, A. Y. S. E. N., & Kebapci, M. A. H. M. U. T. (2002). Diffuse sclerosing variant of papillary thyroid carcinoma with primary squamous cell carcinoma. Journal of endocrinological investigation, 25, 730-734.


