Current Issue : Article / Volume 2, Issue 1
- Research Article | DOI:
- https://doi.org/10.58489/2836-2292/007
Modern instruction in medicine: An overview
Advisor and expert trainer, The National Training and Development Center of the Iraqi Ministry of Health, Member of the advisory council of the International Association of Medical Colleges.
Aamir Jalal Al-Mosawi
Aamir Jalal Al-Mosawi (2023). Advisor and expert trainer, The National Training and Development Center of the Iraqi Ministry of Health, Member of the advisory council of the International Association of Medical Colleges, Journal of Hospital and Clinical Management. 2(1). DOI: 10.58489/2836-2292/007.
© 2023 Aamir Jalal Al-Mosawi, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- Received Date: 31-12-2022
- Accepted Date: 09-01-2023
- Published Date: 17-01-2023
Modern instruction, Medicine, Principles, Concepts, Theories, Methods.
Abstract
Background: Many physicians and other healthcare professionals have jobs at medical colleges and universities, and their job description include instruction and lecturing. In addition, many board-certified physicians are working in university and teaching hospitals have the responsibility of teaching physicians in their residency training. Therefore, not only medical instructors working at medical schools and colleges need to learn about and practice instruction methods. Therefore, there has been an increasing need for physicians to learn about modern instruction methods. The aim of this paper is to provide an overview of modern instruction in medicine.
Materials and methods: The relevant scientific literatures were reviewed with the aim of providing an overview of modern instruction in medicine.
Results: Modern instruction in medicine has become increasingly aiming at facilitating learning and acquiring skills rather than purely giving knowledge. The principles and concepts of modern instruction have been increasingly used by professional institutions during instruction, which is considered by these institutions as âClass trainingâ. The design and organization of modern instruction have been increasingly improved with use of Bloomâs Taxonomy to write learning objectives and to design questions for the exams and assignments. Adopting the ideas of VAK/VARK learnerâs preferences model and using a variety of instruction methods have also contributed to a more effective instruction. Malcolmâs concepts and principles of adult learning (Andragogy) have contributed to advancing modern instruction in medicine. Understanding the major learning theories (Behaviorism, constructivism and cognitivism) enabled the instructors in medicine to develop multiple perspectives into instruction as these theories served as multiple windows in a house that enables looking into the same room and getting different viewpoints from each window. The use of Donald Kirkpatrickâs methods to evaluate instruction has contributed to improving modern instruction through its methodological evaluation. In addition, many other ideas and theories have also contributed to the evolution and advancement of instruction in medicine including Skinnerâs behaviorist model of learning (The operant conditioning), the ideas of John Dewey relevant instruction, constructivist learning theory, Jean Piagetâs cognitive theory, the practical applications of Jean Piaget ideas relevant to instruction, Lev Vygotsky ideasâ practical application ideas relevant to instruction including the zone of proximal development, and the concept of instructional scaffolding suggested by Jerome Seymour Brunerm.
Conclusion: The most important concepts and theories that have contributed to the evolution and development of modern instruction in medicine include Bloomâs Taxonomy, VAK/VARK learnerâs preferences model, Malcolmâs concepts and principles of adult learning (Andragogy), the major learning theories (Behaviorism, constructivism and cognitivism), and Donald Kirkpatrickâs methods of evaluation.
Introduction
Many physicians and other healthcare professionals have jobs at medicalcolleges and universities, and their job description include instruction and lecturing. In addition, many board-certified physicians are working in university and teaching hospitals, and have the responsibility of teaching physicians in their residency training. Therefore, not only medical instructors working at medical schools and colleges need to learn about and practice instruction methods. Therefore, there has been an increasing need for physicians to learn about modern instruction methods.
Learning can be defined as relatively permanent changes in knowledge, skills, behavior or attitudes resulting from particular experiences. Learning can be cognitive, physical, social, or emotional. Permanence is a cardinal feature of learning and temporary changes are not considered learning. Forgotten materials represent a lost change can not be regarded as being learnt. To ensure the permanence of change during instruction, it is important to transfer the taught materials to future practice. After instruction, learners should be able to use the acquired knowledge or skills in their practical experience. Instruction is the instructor’s efforts, while learning is what learners achieve from their efforts. Therefore, learning is not referring only to the experiences and what are encountered during instruction because important part of learners’ efforts may be achieved outside the instruction rooms. The instruction environment, and the number of learners, can affect learning, and how instruction should be conducted. The learning materials are generally presented as curriculum content and the skills expected to be learned during instruction. The initial preparedness of the learners to cope with or to get benefit from the activities has an important influence on learning [1-6].
The aim of this paper is to provide an overview of modern instruction methods in the field of medicine.
Materials and methods
The relevant scientific literatures were reviewed with the aim of providing an overview of modern instruction methods in medicine.
Results
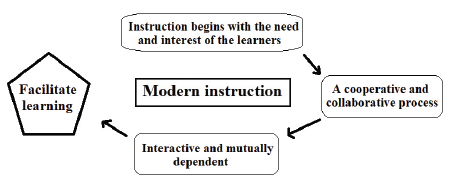
Modern instruction in medicine has become increasingly aiming at facilitating learning and acquiring skills rather than purely giving knowledge.
The principles and concepts of modern instruction have been increasingly used by professional institutions during instruction, which is considered by these institutions as “Class training”.
The design and organization of modern instruction have been increasingly improved with use of Bloom’s Taxonomy to write learning objectives and to design questions for the exams and assignments.
Adopting the ideas of VAK/VARK learner’s preferences model and using a variety of instruction methods have also contributed to a more effective instruction.
Malcolm’s concepts and principles of adult learning (Andragogy) have contributed to advancing modern instruction in the field of medicine.
Understanding the major learning theories (Behaviorism, constructivism and cognitivism) enabled the instructors un the field of medicine to develop multiple perspectives into instruction as these theories served as multiple windows in a house that enables looking into the same room and getting different viewpoints from each window.
The use of Donald Kirkpatrick’s methods to evaluate instruction has contributed to improving instruction through its methodological evaluation in modern times.
In addition, many other ideas and theories have also contributed to the evolution and advancement of instruction in medicine including Skinner’s behaviorist model of learning (The operant conditioning), the ideas of John Dewey relevant instruction, constructivist learning theory, Jean Piaget’s cognitive theory and the practical applications of Jean Piaget ideas relevant to instruction, Lev Vygotsky ideas’ practical application ideas relevant to instruction including the zone of proximal development, and the concept of instructional scaffolding suggested by Jerome Seymour Brunerm.
Discussion
Modern instruction in the field of medicine has become increasingly aiming at facilitating learning and acquiring skills rather than purely giving knowledge [2-9].
The principles and concepts of modern instruction have been increasingly used by professional institutions during instruction, which is considered by these institutions as “Class training” [2, 4].
Modern instruction methods have been increasingly used to maximize good learning experience.
Other factors that contribute to improvement of instruction in medicine include the recognition that the most essential instructor’s quality and role is the quality of being expert in the subject being taught, and the ability to take the role of the more knowledgeable expert can not be compensated by any other personal qualities.
The importance of making revision of the learnt materials has been increasingly emphasized in instruction.
Other factors that contribute to improvement of instruction in the field of medicine also include the emphasis on teaching participants what they have to remember and what to expect at the exam [10, 11, 12].
Modern instruction in medicine can be preceded by a pre-test which can help in the evaluation of the acquisition of knowledge after instruction. The pre-test is generally followed by introductory talks and activities that describe the main aims of the course, the learning objectives, the main instruction methods, and also the accreditation of the training course when relevant. Before starting the instruction modules or units, instruction for postgraduate doctors, instruction is generally preceded by an ice breaking activity (Box-1).
Box-1: Ice breaking activity |
It has become an orthodox to begin instruction and lectures for postgraduate students with an ice breaking activity where participants introduce themselves and give a brief account about their experiences relevant to the theme of instruction. Ice breaking activity is considered a facilitation technique which helps the participants to know each others, to adapt to the instruction environment. |
Common objectives |
1-Making the participants relax and initiate communication. 2-Getting attention and involve all participants rapidly. 3-Remove barriers and clears mind blocks. 4-Giving fun and humor to the atmosphere. |
Telling the participants about the factors associated with effective participation and more benefits from instruction has been increasingly practiced during modern instruction in the field of medicine (Box-2).
Box-2: Telling the participants about the factors associated with effective participation and more benefits from instruction has been increasingly practiced during modern instruction in the field of medicine |
To feel free to ask a question when you need, and ask for an example or more clarification for a better understanding. To feel free to share their understanding. To make correlation between the learnt knowledge and skills and their work and how they can improve them performance using them. To think of the learnt knowledge and skills that they can pass to their colleagues. To respect the thoughts and suggestions of other participants. |
An important purpose of modern instruction process is to facilitate learning, and to make learners motivated to seek new knowledge, skills and behaviors. Instruction methods are designed to maximize good learning experience. Modern instruction methods have been increasingly used by professional institutions during instruction is generally called “Class training” (Figure-1A).
The design of modern instruction in medicine has been improved by adopting the features that make instruction more effective (Box-3).
Box-3: The features that make instruction more effective |
1-Making learning materials consequential as it will be easier to understand and to remember. Instruction materials can be made consequential by: A-Providing an overview of the materials to be presented at the start of instruction, and this is usually achieved by providing the syllabus of instruction. B-Distributing a printed paper summarizing the general ideas of the instruction materials (Handouts and worksheets). C-The use of familiar examples. D-Organizing the presented information logically. |
2-Making the knowledge learned during instruction easily transferable to the work site. This can be achieved by: A-Maximizing the similarities between instruction materials and what the learners will experience in their practice. B-Providing a time for adequate practice. People learn better by doing, therefore; it is important to provide practice as realistic as possible. |
3-Motivating the learners by: A-Explaining why instruction is important and how it will benefit the learner. B-Reinforcing immediately correct responses during instruction. C-Giving extra-marks to the participant who volunteer to summarize the materials learnt during an instruction session or an instruction day. |
4-Making the participants know what is necessary to complete the instruction successfully and pass the necessary tests. |
5-Motivate learning by giving extra-marks the participant who volunteer to summarize the materials learnt during an instruction session or an instruction day. |
The design of modern instruction in medicine has also been improved by considering the participants’ feedback which is received at the end of instruction modules (Box-4) [13, 14].
Box-4: Participants’ feedback which are received at the end of instruction modules can help in improving instruction |
What is in your opinion, the one most important thing you have learned today? What is the topic that you liked most today? Is there a thing comes to your mind and you wanted to learn more about it. What is the topic that you didn’t like? What is the thing that gave you some difficulty? What thing you would like to know more about it? |
Instruction methods commonly used during instruction in medicine are shown in figure-1B.
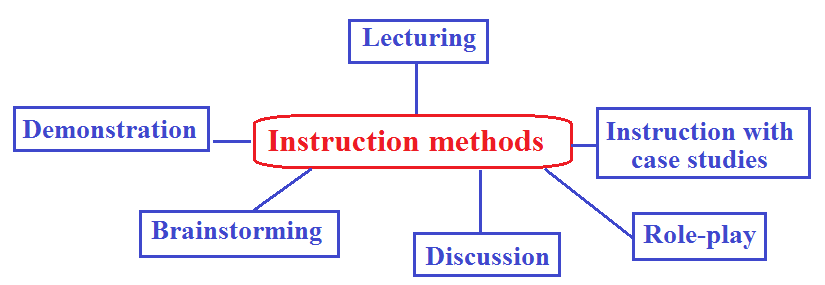
Each of these popular instruction methods has advantages and disadvantages. However, depending on the situation, each method can be a valuable tool for the acquisition of knowledge and skills.
Lecturing or explaining is one of the most popular instruction methods. During a traditional lecture, the instructor usually talks and the participants listen with or without taking notes. Lecturing is the process of instruction by giving spoken explanations of the subject to be learned. Lecturing is often accompanied by visual aids to facilitate learning.
Lecturing has the advantage that learning materials can be covered easily and quickly, but learning during lecturing can be associated with lack of interaction and high likelihood of boredom.
Understanding some of the misconception associated with the instruction method of lecturing has contributed to improving modern instruction medicine. It is pity to observe many who lack the experience of lecturing, make a lecture by copying texts from books or other sources, thus converting this instruction method of lecturing into something more like a book reading. Many experts suggested that instead of reading a text brought from books, articles and other sources, it will be more convenient and time saving to ask the audience to read the chosen text or article. Therefore, in order to avoid the unnecessary practice of book or article reading instead of lecturing, a lecture should include at least 10 references. For lectures in the field of applied sciences like medicine, at least seven of the references should be scientific journal articles, and the use of books as a reference is preferably limited to three or less.
Modern instruction in the field of medicine has been improved by adopting the features that make lecturing more effective (Box-5).
box-5: Features that make lecturing more effective |
APPROPRIATE PREPARATION OF A LECTURE INCLUDE: Organizing the ideas of a lecture by selecting a title that conveys clearly what the lecture is all about, and giving an overview about the topics of the lecture with a concise overview of the new information presented during the lecture. Relating new content to prior knowledge. Organizing and elaborating new information. Reducing boredom by asking questions, inviting questions and allowing discussion. |
EFFECTIV ELECTURING DURING INSTRUCTION demands adequate preparation before lecturing, keeping the attendance with the instructor through adequate eye contact as possible, speaking clearly, and involving the participants thorough encouraging questions. Effective lecturing during instruction also demands keeping the attendance focused on the presented materials by presenting the topics and materials in a logical sequence, bridging each topic to the next, and by the use of visual aids. |
Appropriately using role-playing instruction method during instruction can help in the achievement of effective learning through making the participants practice skills they have acquired, and demonstrating their knowledge and understanding of instruction materials. In clinical sessions, medical students play their future role as doctors, and learn how to take history and perform a physical examination. This instruction method is also appropriate in teaching students of medicine and postgraduate physicians counseling skills, and it can be used in clinical sessions and consultation clinics, where the consultant allow the trainees to play their future role as a consultant and provide counseling.
It has been disturbingly observed that many learners in the field of medicine, both undergraduate and postgraduate, may have satisfactory information acquisition in their fields of study, but fail to use it appropriately when it come to clinical practice. Instruction with case studies has been used to encourage learners to adopt deep learning approaches and enhance understanding which help in establishing and creating experience.
Modern instruction in medicine has also been improved by adopting the features that make instruction with case studies more effective.
In the field of medicine, case studies used during instruction should be real cases and supplemented by questions that help in understanding and expanding to the relevant knowledge. Case studies improve retention, recall, and application of knowledge in real practice situations, and gaining the experience with the diagnosis and management of conditions that have not been encountered by the students or trainee.
Demonstration as a method of instruction is generally practiced by showing how to do it, for example how to reach a clinical diagnosis. It is based on making impersonal experiences of memorization become like a personal experience. It helps to raise participants’ interest and reinforce memory retention because they provide connections between facts and real applications of those facts. For example, when teaching how to reach a diagnosis of a clinical problem through considering various differential diagnoses and excluding the less relevant diagnoses.
Discussion is an instruction method that is generally more suitable for instruction provided for postgraduate physicians. It is an active learning process by talking with each other and listening to other points of view. In this instruction method, the instructor describes briefly a topic or problem and invites participants to comment. One of the advantages of this method is enabling the instructor to judge the interest of the participants in the topic and the opportunity to stimulate interest. However, discussions may not cover all the points intended to be covered and dominant participants may take over and do not allow hesitant participants to speak [14-19].
Brainstorming is an instruction method that is suitable for postgraduate physicians. It is generally aiming at stimulating participants’ creativity to help them in finding possible solutions for a specific problem. It is initiated by presenting a main statement which defines clearly the problem, and asking participants to feel free to offer any solution that can help in identifying the roots of the problem, and thus facilitating a solution. At the beginning, all the spontaneous new ideas are taken and listed without allowing criticism. Thereafter, the ideas are evaluated with aim of taking the more logical and practical suggestions.
Brain storming method was first suggested by Alex Faickney Osborn (Figure-2A) in his book “Applied Imagination, Principles and Procedures of creative thinking” (Figure-2B).
Alex Osborn thought that the two principles that could contribute to "ideative efficacy," are: Defer judgment and reach for quantity.
Alex Osborn used four general rules (Box-6) to practice brainstorming with aim of reducing social inhibitions among the participants, stimulating idea generation, and enhancing overall creativity of the participants.


Box-6: Osborn’s four rules for brainstorming |
1-An initial emphasis on quantity to facilitate the emergence of a solution for the presented problem. The more the generated ideas the higher the chance of finding an effective solution. 2-An initial withholding of criticism to encourage the participants to focus on increasing the umber of ideas. Therefore, during the early stage, judgment is suspended to make the participants feel free to generate unusual ideas that may prove later to be useful. 3-Welcoming wild ideas to obtain a satisfactorily long list of suggestions, and allowing the emergence of new perspectives which may lead to better solutions. 4-Combining ideas and improving them. |
Alex Osborn suggested beginning the method by asking one specific question and not multiple questions. The question should aim at defining and solving a problem that requires the generation of ideas rather than judgment.
Learning is a self-activity, and modern instruction in essence aims at facilitating learning rather than purely giving it. Learners differ in their rate of learning, and superior learning during instruction can be achieved by doing. Positive reinforcement enhances learning. Barriers to learning during instruction include learner’s personality, the perception of instruction as a waste of time, and lack of reward and incentive system [20, 21].
Understanding the factors affecting instruction effectiveness (Figure-3 and Box-7) has also contributed to improving modern instruction in the field of medicine.
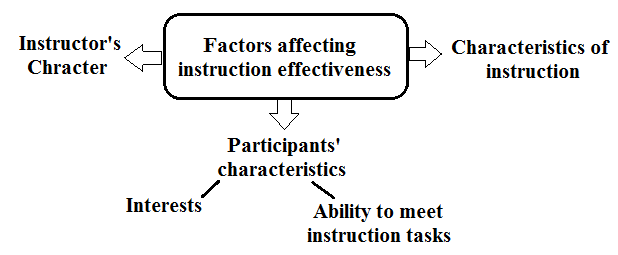
Box-7: Factors affecting instruction effectiveness |
INSTRUCTOR’S CHARACTERS |
1-Instructor’s Knowledge, enthusiasm, and preparation before the instruction. 2-Affability and interest in and respect for learners. 3-Encouragement of participants’ ideas. 4-Availability for advice, feedback, and support. |
INSTRUCTION CHARACTERISTICS |
1-Organization of instruction with use of a syllabus describing the instruction plan. 2-Learning objectives. 3-Fair assessments using a variety of tests. 4-The value of the scientific materials (curriculum). 5-Instruction environment and openness to questions and discussion. 6-Instruction management and adherence to instruction objectives. 7-Motivation of learners and inspiration of interest in instruction and its content. |
The instructor cannot control all the factors affecting instruction effectiveness especially when working as a part of a team. In some circumstances, instruction materials, and textbooks are determined by a committee rather by the instructor. The instructor may teach in courses that are a part of a degree program in which certain objectives, determined by the institution granting the degree. However, the instructor is expected to try to maximize input into the controllable factors that influence instruction outcomes and its assessment.
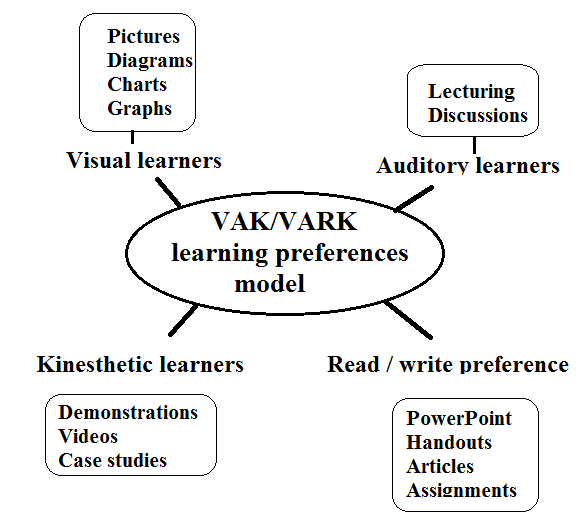
VAK/VARK learner’s preferences model has also contributed to the development and improvement of modern instruction in the field of medicine. The VAK model suggests that people vary in their learning orientation, and learners' preferences include visual learning, auditory learning, and kinesthetic learning. Accordingly, instructors have to use various approaches to engage all participants with various learning styles.
Visual learners prefer pictures, diagrams, charts, graphs, flow charts. Therefore, this learning preference is also called “Graphic (G) preference)”.
Auditory learners prefer receiving information by listening. Lecturing and discussions are more effective with such learners.
Kinesthetic learners prefer using experience and practice. Instruction methods that are more useful for kinesthetic learners include demonstrations, simulations, videos, case studies, and practice.
Many learners are multimodal in their learning preference and have two, or more almost-equal learning preferences.
Neil D. Fleming (Figure-4A) added a fourth learning preference which is Read/write (R), and the VARK model (Figure-4B) emerged (Visual, Aural, Read/write, and Kinesthetic sensory).

Fleming introduced the VARK model while working as an inspector for the New Zealand education system. Fleming thought that some eminent teachers could not reach some students while other less reputed teachers could. Therefore, he introduced the VARK model based on his experiences, and work with students and teachers at Lincoln University.
Read/write preference learners need information to be displayed as words and text-based input and output (reading and writing) in all its forms including PowerPoint, handouts including worksheets, articles, and assignments [22,23].
The evolution of modern instruction in the field of medicine has been associated with the emergence of the fundamental principles of modern instruction (Box-8).
Box-8: The fundamental principles of modern instruction |
LEARNING DURING INSTRUCTION IS AN EMOTIONAL AND AN INTELLECTUAL PROCESS INVOLVING CHANGING BEHAVIOR WITH EXPERIENCE |
Learners are more willingly accepting and using concepts that have meaning to them and are relevant to their lives, work needs and problems. Learning varies within a group of learners. Learning during instruction may involve changing ways of believing, thinking and acting. Therefore, learning is not always a pleasant experience for a learner. Learners’ background of knowledge and experiences are affluent resource for problem solving and learning. Learners tend to adopt their individual ways of learning and solving problems. However, when Learners are exposed to others’ methods, they may refine their ways to become more effective. Learning during instruction is maximized when the learners understand and express what they think and feel. |
INSTRUCTOR’S ROLES IN FACILITATING LEARNING DURING INSTRUCTION: MAXIMIZING LEARNING POTENTIAL |
A-Encouraging learners to be active. B-Clarifying the personal nature of learning during instruction. C-Accepting differences, recognizing the learners’ right to make mistakes, and tolerating limitations and imperfection. D-Encouraging self-openness and self-trust. E-Encouraging the learners’ feeling of being respected and accepted. F-Accepting arguments. |
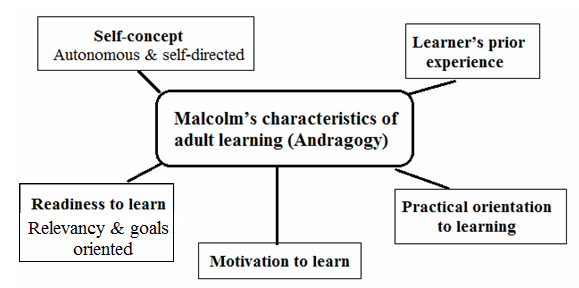
Malcolm’s concepts and principles of adult learning (Andragogy) have also contributed to advancing modern instruction in the field of medicine. According to Malcolm (Figure-5), Andragogy is the art and science of adult learning. and it encompasses all forms of adult learning. In Greek, andragogy means man-leading, and, pedagogy means child leading. Pedagogy is a teacher directed approach of instruction.

In 1980, Malcolm suggested four characteristics of adult learners that are different from the characteristics of child learners (Box-9 and figure-5B). In 1984, Malcolm suggested a fifth characteristic. In 1984, the ideas of Malcolm suggested four principles of adult instruction (Box-10).
Box-9: Malcolm’s characteristics of adult learners |
Adults’ self-concept which makes them autonomous and self-directed and need to be respected and treated as self-directed individuals. Adult accumulated and growing experiences represent an important resource for learning. Adults’ readiness to learn because they are relevancy and goals oriented. Adults’ practical orientation to learning makes them want to apply their knowledge with the perspective of immediate application rather than the postponed perspective of application. Adults’ internal Motivation to learn (1984): They need learning to be enjoyable and gives them satisfaction. Adult learners also need to have a choice over what they learn. |
Box-10: Malcolm’s four principles of adult instruction |
Adults have to be involved in planning and evaluation of their instruction. Experience (including mistakes) provides the basis for the learning activities during instruction. Adults are most interested in learning things of immediate relevance and impact to their job or personal life. Adult learning is problem-centered rather than content-oriented. |
Malcolm’s ideas practical applications in instruction include:
It is important to explain the reasons why specific things are being taught during instruction.
Instruction should be more task-oriented instead of memorization.
Instruction should consider the differences of the learner’ backgrounds, and use various instruction methods, learning materials and activities.
Adults are self-directed; therefore, instruction should attempt to make them discover knowledge with guidance and supervision without totally depending on the instructor.
The major learning theories including behaviorism, constructivism and cognitivism (Figure-6) have also contributed to the advancement of modern instruction in the field of medicine.
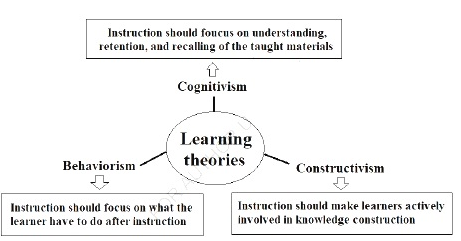
Learning is a change in mental association and behavior due to certain experience. There are several theories of learning including theories of behaviorism, constructivism and cognitivism. Understanding learning theories enables the instructor to develop multiple perspectives into instruction. Therefore, learning theories are like multiple windows in a house that enables looking into the same room to get different viewpoints from each window.
Cognitive learning occurs through the acquisition of knowledge and skills by mental or cognitive processes and information processing.
In cognitive learning, the learner learns by listening, watching, reading, or experiencing and then processing and remembering the information.
Cognitivism is a learning theory focusing on how information received, organized, stored and retrieved by the mind. Cognitivism views the mind as an information processor. Accordingly, instruction should focus on achieving three goals:
1-Understanding
2-Retention
3-Recalling
Cognitivism emphasizes that better retention and recall of information can be achieved through the use of a well-organized and sequenced instruction processes, and presenting the information in a consequential and easily understandable way. Better understanding can be achieved by activating prior knowledge by beginning instruction by a review quiz and arranging the information into comprehensible parts, and using graphics.
Retention of information can be improved with use of visual aids and mnemonics like SMART objectives (Specific, Measurable, Achievable, Relevant, and Time-bound). Cognitivism emphasizes that learning involves recall of stored information, and learning occurs when the learner can recall stored information.
Behaviorism theory focus on behavior instead of thought during instruction and suggests making behavior changes in the learner by repetition and reinforcement with focusing on what the instructor wants the participants to do. However, for a beginner (e.g. a medical student), focusing on the gains in knowledge (Cognitive approach) is necessary, and it is more important to be able to describe how to perform the procedure than actually be able to do it. Therefore, it would be better to think of both approaches when planning instruction.
Constructivism theory emphasizes that using learners’ prior knowledge as the starting point for new learning can be associated with more effective learning. It focuses on the inner thoughts of learners, and how they actively construct knowledge out of experiences, and thus it suggests that instruction have to make learners actively involved in the process of knowledge construction as possible rather than just receiving information. Learning is best achieved by guiding problem solving. Therefore, constructivist instruction encourages critical thinking, and creates motivated and independent learners that can build knowledge by doing or practicing.
Bloom’s Taxonomy has also contributed to the evolution and development of modern instruction in medicine. The cognitive domain of learning and instruction has been the primary focus of the majority of traditional instruction methods. It is frequently used to structure curriculum learning objectives, assessments and activities. It was originally suggested by Benjamin Bloom (Figure-7A), who was the chair of the committee of educators who proposed taxonomy of educational objectives based on the classification of educational goals.

They published the first volume of the standard taxonomy of educational objectives. The taxonomy aimed at promoting higher thinking in education such as analyzing and evaluating. In 1956, Bloom edited the first volume of “Taxonomy of educational objectives: the classification of educational goal”. The publication described a classification of learning objectives (Bloom's taxonomy) which became an important tool for developing instruction and educational curriculum. In the original version of Bloom’s taxonomy, the cognitive domain classified thinking and learning into six levels with six levels of objectives (Figure-7B and Box-11) that can be practically used to create learning objectives for instruction.

Box-11: Bloom’s six levels of objectives |
Remembering involves retrieving, recognizing, and recalling knowledge (facts, terms, and basic concepts) for long term memory without necessarily understanding their meaning. Remembering is necessary in acquiring knowledge of specifics such and knowledge of classifications and categories. Understanding or comprehending involves constructing meaning of facts and ideas from oral, written, and graphic messages. Understanding can be shown by the ability to interpret, explain, infer, compare, and summarize by organizing the main ideas. Applying the learnt knowledge (facts, techniques and rules) to perform or conduct something. Analyzing information by dividing it into parts, and determining how the parts are related, and identifying causes, and making inferences and finding evidence to support generalizations. Evaluating involves: Making judgments based on criteria and standards. Presenting views and opinions, and supporting them by information. Evaluating the validity of ideas, or quality of work based on a set of criteria. Synthesizing or creating a structure or pattern from diverse elements by putting parts together to form a whole. Synthesizing involves making a unique message or statement and making a plan. |
In the 2001 revised edition of Bloom's taxonomy, the levels were a little different and included remembering, understanding or comprehending, applying, analyzing, evaluating, and creating rather than synthesizing. The six cognitive levels are generally hierarchical and begin with lower order thinking skills to higher order thinking skills. Learning on higher levels generally demands gaining prerequisite knowledge and skills at lower levels. Bloom's taxonomy can be used as backbone of instructional materials, and can also be used for organizing the taught knowledge and skills. Bloom's taxonomy can also be used as a tool to design questions for the exams and assignments.
According to Bloom’s taxonomy:
The participant needs to remember the concept before being able to understand it.
The participant needs to understand the concept before being able to apply it.
The participant needs to analyze the concept before being able to evaluate it.
The participant needs to thoroughly evaluate a concept before being able to create an accurate conclusion or using it in performing something.
When introducing a new concept, the participants need to remember, understand, and apply the concept before moving to the higher order skills such analyzing, evaluating, and creating.
The cognitive domain levels help the instructor to write measurable and observable learning objective statement to describe what the participants will be able to do at the end of instruction unit or module [24, 25].
Modern instruction in the field of medicine has been improved with the use of Donald Kirkpatrick (Figure-8A) four levels of evaluation (Figure-8B and Box-12).
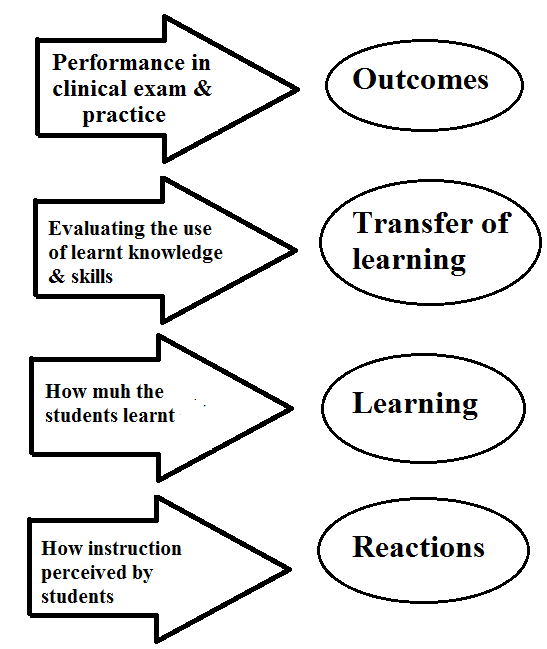
Box-12: Donald Kirkpatrick's four levels of evaluation |
LEVEL 1 EVALUATION: REACTIONS |
Participants' reactions have an important relation with learning and instruction. However, a positive reaction does not guarantee learning and successful instruction, but a negative reaction almost certainly reduces the possibility of significant learning achievement and successful instruction. This level evaluates how the participants perceived the instruction, and how they felt about it. Participants' reactions evaluation is generally performed using a feedback form. It is a simple measure of the level satisfaction of the participants: Did the participants like the instruction? Did the participants consider the materials relevant to them and important? |
LEVEL 2 EVALUATION: LEARNING |
This level evaluates the amount of participants’ learning by measuring the acquisition of the content in term of gain in knowledge and skills, and if relevant and possible, the change in attitude. Ideally, learning evaluation is performed formally by conducting a pretest (before instruction), and post-test (after instruction), and comparing the two tests. |
LEVEL 3 EVALUATION: TRANSFER OF LEARNING |
This level evaluates if the knowledge, and/or skills learned during instruction are useable in the practical experience of the learner who is in this setting a medical student or a postgraduate physician. For medical students, this evaluation can be performed during the clinical sessions following instruction. For postgraduate physician, this evaluation level is usually conducted by the clinical supervisor after instruction by observing the trainees in their workplace. |
LEVEL 4 EVALUATION: RESULT (OUTCOMES) OF INSTRUCTION |
For medical students, this evaluation can be performed during the clinical examinations following instruction. For postgraduate physician, this evaluation level is usually involves assessing the success of trainees in making service improvement, and reducing errors in his/her practice. |
The practice of instruction effectiveness evaluation has also contributed to advancing modern instruction in the field of medicine.
Instruction evaluation is generally performed formally by the institution at the end of the instruction “Final summative assessment” and is usually made by a peer instructor of equivalent professional and academic level by filling an evaluation form. Early formative assessment is preformed in case of instruction courses of two weeks duration or more with the aim of giving the instructor the opportunity to respond to suggestions for improvement.
Early Formative assessment of participants’ learning is a part of instruction process, and it provides an earlier understanding of the participants learning. It is performed through observation of learners’ acquisition of new knowledge and skills, and their understanding of a new concept; quizzes; making presentations; activities; effective questioning techniques to the determine depth of understanding of a concept; and assignments designed to target certain skills.
End of session or instruction day form can be used to assess the learned knowledge, and uncovers possible knowledge gaps. Questions in the form my include:
A-What is the one most important thing you have learned from this session?
B-What is the thing that gave you some difficulty?
C-What thing you would like to know more about it? [10, 11, 12, 26, 27].
Many other ideas and theories have also contributed to the evolution and advancement of instruction in medicine including Skinner’s behaviorist model of learning (The operant conditioning), the ideas of John Dewey relevant instruction, constructivist learning theory, Jean Piaget’s cognitive theory, the practical applications of Jean Piaget ideas relevant to instruction, Lev Vygotsky ideas’ practical application ideas relevant to instruction including the zone of proximal development, and the concept of instructional scaffolding suggested by Jerome Seymour Brunerm.
Skinner’s Behaviorist model of learning (The operant conditioning)
Burrhus Frederic Skinner (Figure-9) was probably the first to bring the attention to the similarities between operant conditioning in the original research on tame laboratory rats and operant conditioning in humans. According to Skinner’s ideas it is possible to strengthen desired behavior using operant conditioning. Operant conditioning is a learning process associated with likelihood that a specific behavior is increased or decreased through positive or negative reinforcement whenever the behavior is made; in result the individual associates the satisfaction or dissatisfaction with the positive or negative reinforcement.

During instruction operant conditioning begins with the idea that certain consequences tend to make certain behaviors happen more frequently; e.g., if an instructor compliments (reinforcement) a participant for a useful comment made (The operant or the learned behavior) during a discussion, there is more chance for more comments to be made in the future.
Accordingly, the participants can be motivated and encouraged by giving a strong reason to do the desired action or to accomplish something. Skinner has been respected for suggesting what was considered a much-needed scientific approach to the study of human behavior. However, he has also been criticized for applying findings based largely on animal experiments to human behaviors. Skinner’s operant conditioning is considered the most common version of behavioral motivation approaches.
Reinforcement is the fundamental concept of behaviorism, and it is considered the primary process that forms and controls behavior.
Positive reinforcement is the strengthening or reinforcement of behavior by the occurrence of an event or action such as praise after a behavior.
Negative reinforcement is the strengthening or reinforcement of behavior by the removal or avoidance of an unwanted event or experience. The behavior of using an umbrella is negatively reinforced by the cessation of rain.
Skinner thought that human actions are affected by results of previous actions, events or experiences. Therefore, if a previous a behavior resulted in an undesirable outcome, the behavior will not be repeated. Whereas, if a previous behavior resulted in a desirable outcome, the behavior is likely to occur again in the future. Reinforcement is more effective if it comes immediately after certain operant behavior. For example, the behavior of making a useful comment during instruction is more likely to be reinforced by immediate praise.
Operant conditioning affects motivation by encouraging intrinsic (internal) motivation, to the extent that the reinforcement for an activity is the activity itself. For example, when a learner reads a book for enjoyment of reading alone, he is reinforced by the reading itself, and reading is considered to be intrinsically motivated. Operant conditioning is not relevant to all forms of learning.
According to Skinner’s ideas, effective instruction may be based on positive reinforcement which he considered more effective at changing and establishing behavior than punishment. Trainees and learners learn mainly from being punished is how to avoid punishment. For example, if a trainee or a learner is forced to practice something, practicing will be associated with punishment and thus learns to hate and avoid practicing that thing. Instructors can modify trainees’ behavior, and failure of instruction could be attributed to the lack of instructor’s in-depth understanding of instruction and learning.
Skinner’s ideas about instruction suggested that without having adequate knowledge of the science of instruction, inappropriate methods and procedures can be used including:
The use of techniques that may lead to escape and avoidance and undesirable emotional effects.
Relying on telling and explaining.
Failure to assign learning tasks and to provide positive reinforcement adequately.
The ideas of John Dewey (Figure-9) relevant and instruction
1-Learners learn primarily by building on their own knowledge.
2-Instructors should designand modify the curriculum to fit participants’ prior knowledge and interests.
3-A curriculum needs to focus on the activities and responsibilities that a course participants or learners will practice in the future.
Dewey’s ideas suggested that instruction must connect with and enlarge experience and thus instructors have to take the role of exploration of thinking and reflection [2, 3, 4].Box-13 summarizes John Dewey ideas about instructors’ qualities.
Constructivist learning theory or constructivism is a learning model suggests that participants can learn through guided experiences and reflecting upon those experiences. The participants are encouraged to actively engage in the process of learning to develop knowledge. The process is more democratic and participants-centered. Instructors take the role of facilitator, rather than lecturer. In the constructivism model, instructors’ main role includes promoting critical thinking and creates independent learners who develop their own understanding of new knowledge. Models of constructivist learningtheory differ about how much a learner constructs knowledge independently, comparedto how much they take. However, all models of constructivist learning focus on learner’s thinking rather than learners’ behavior, but they have distinctly different implications for instruction.
There are two main varieties of constructivism; psychological constructivism and social constructivism. Psychological constructivism and social constructivism suggest different approaches for effective instruction most effectively.
Box-13: John Dewey ideas about instructors’ qualities |
There are scholars who have [the knowledge] in a marked degree but who lack enthusiasm for imparting it. To the natural born teacher learning is incomplete unless it is shared. |
An instructor should have the inclination and passion for intellectual growth and a natural desire to communicate knowledge with others. |
It is not enough for an instructor to be a lifelong learner of the techniques and the science of instruction. An instructor should always aspire and seek to share what knows with others in a learning community. |
An instructor should have the ability to observe and respond to the movement of the mind with sharp awareness of the signs and quality of the responses the participants exhibit about the instruction materials. |
Instructors who have never studied the art of instruction, but they were extraordinarily good instructors. Dewey explained that such instructors have a quick, sure and persistent sympathy with the operations and processes of the mindsthey are in contact with. |
Good instructors who didn’t study the art instruction have a natural and genuine awareness of the complexities of mind-to-mind transfer, and have the intellectual strength and determination to recognize the successes and failures of the mind-to-mind transfer process, and how to appropriately repeat or correct it in the future. |
Dewey’s ideas suggested that instructor personal inherent qualities are the most important attributes of good instructor as the acquired pedagogical skill can not totally compensate the deficiency of the personal traits needed to be most successful in the profession ofinstruction. |
Psychological constructivism emphasizes the independence of learners’ thinking, while social constructivism gives attention to learners’ need for social connections while learning. The main idea of psychological constructivism is that learning is achieved by mentally organizing and reorganizing new information or experiences. The organization occurs partly by relating new experiences to prior knowledge that is already meaningful and well understood.
Jean Piaget’s cognitive theory
Jean Piaget (Figure-10) describedlearning as interplaybetween two mental activities called assimilation and accommodation. According to Piaget, assimilation and accommodation work together to enrich thinking and to create cognitive equilibrium. Assimilation is the interpretation of new information in terms of pre- existing concepts, information or ideas. Accommodation is the revision or modification of pre-existing concepts in terms of new information or experiences. It occurs alongside assimilation.
Piaget ideas suggested the occurrence of two types of adaptations during learning. Assimilation is learner’s response to a new event based on an existing schema, and in accordance with individual needs or conceptions.
Accommodation is learner’s modification to an existing schema or learner s formation of a completely new schema to deal with a new experience or event.
Cognitive equilibrium is a balance between reliance on prior information and openness to new information. It consists of an ever- growing collection of mental representations for objects and experiences. Piaget called each mental representation a schema.
A schema is a concept accompanied by an elaborated mixture of vocabulary, actions and experiences related to that concept. A schema is the mental framework of structured cluster of concepts that is created as a result of the interaction with physical and social environments. Schemata are:
Critically important building block of conceptual development.
Constantly in the process of being modified or changed.
Modified by on-going experiences.
A generalized idea, usually based on experience or prior knowledge.
According to Piaget ideas, instruction have to be learner-centered and constructivist to some extent with understanding that participants are adding new concepts to prior knowledge to construct, or build understanding. Piaget ideas suggested that instructors have to consider the learners individual qualities and attitudes during curriculum planning, and add learners thought into the curriculum. Piaget ideas also suggested that instructors have to nurture and sustain learners’ curiosity, and involve learners’ emotions and create a learning environment which makes participants feel safe. According to Piaget’s work and ideas, participants can learn by expanding their knowledge and experiences accumulated from infancy to adulthood which are necessary for learning.
The thoughts of Dewey and Piaget played crucial role in the development of informal education. The theories of Dewey and Piaget became part of the movement of progressive education.
Social constructivism (Socio-cultural theory) emphasizes the importance of the relationships and interactions between a learner and the instructors who are more knowledgeable or more experienced. The social constructivist theory suggests that learning is like assisted performance. During learning, knowledgeor skill from the expert who is skilled and motivated to teach can arrange experiences of the learner to allow the learner to practice crucial skills or to construct new knowledge. Lev Vygotsky (Figure-11A) suggested that learners’ thinking is influenced by relationships with the more knowledgeable or expert and constructs knowledge better with social interaction with more knowledgeable and expert people. Vygotsky called the difference between what the learner can do alone and what can not do without assistance, the zone of proximal development (Figure-11B).


Lev Vygotsky ideas’ practical application about instruction included [2, 3, 4]:
1-Learning should begin by focusing on fields within learners’ zone of proximal development where instruction is most beneficial because it is just beyond participants’ current level of capability. With progressive learning the zone of proximal development will expands allowing the learners to handle progressively more complex topics.
2-If learning continues within learners zone of proximal development, boring will ensue because the learners experiencing things that can do or learn independently, and can not perceive the need for instruction.
3-If the instructor begins instruction with contents that are difficult to achieve even with assistance, the learners will give up, and there will be a negative impact on the learners self confidence.
4-The people who help others learn should be more knowledgeable and expert to be capable of providing the necessary support and the social interaction which is believed to affect high order thought processes.
Instructional scaffolding
Jerome Seymour Bruner thought that learners could usually learn more than was traditionally expected as long as they were given appropriate guidance and resources. Instructional scaffolding is the phrase that Jerome Seymour Bruner (Figure-12) used to describe the support that learners should be given as they learn.

Instructional scaffolding literally means a temporary framework like the ones used to construct buildings, which allows a much stronger structure to be built within it. Bruner emphasized the importance of providing guidance in the proper way and at the appropriate time. When scaffolding is provided correctly, learners appear to be more competent and they learn more. Bruner's work also suggested that a learner is capable of learning any material provided that the instruction is organized appropriately. Scaffolding is the support needed to help participants in achieving the learning objectives including the interactions aimed at guiding learning.
Scaffolding is a strategy than can be used by an experienced instructor to help less experienced participants when the experience difficulty. The process of scaffolding includes dividing learning into steps with the provision of guidance and monitoring. Guidance by providing step by step clear direction explaining what the participants have to do to achieve the objectives of a learning activity.
Bruner also suggested the use of the spiral curriculum, an instruction approach in which each subject or skill area is revisited at intervals, at a more sophisticated level each time. First there is a basic knowledge of a subject, and then more sophistication is added, reinforcing principles that were first discussed. Bruner emphasized that learning is stimulated by creating interest in the material rather than by tests or punishment. Learners learn best when the presented knowledge are interesting [2, 3, 4].
Conclusion
The most important concepts and theories that have contributed to the evolution and development of modern instruction in the field of medicine include Bloom’s Taxonomy, VAK/VARK learner’s preferences model, Malcolm’s concepts and principles of adult learning (Andragogy), the major learning theories (Behaviorism, constructivism and cognitivism), and Donald Kirkpatrick’s methods of evaluation.
Acknowledgement
Some of the figures and boxes in this book were included in the author’s previous publication, but the author has their copyrights,
References
- Al-Mosawi AJ. Principles of training and development for physicians .1st ed., Saarbrücken; LAP Lambert Academic Publishing: 2014 (ISBN: 978-3-659-53092-0). Doi:10.13140/rg.2.1.1173.4803
- Al-Mosawi AJ. An accredited training of the trainers (TOT) training course. 1st ed., Saarbrücken; LAP Lambert Academic Publishing: 2017 (ISBN: 978-3-659-88198-5).
- Al-Mosawi AJ. Essential training knowledge for physicians working in the field of professional training and development, and medical schools’ instruction. Research and Reviews on Healthcare: Open Access Journal (ISSN: 2637-6679) 2019 November 25; 4; 3: 347-367.Doi:10.32474/RRH OAJ.2019.04.000187
- Al-Mosawi AJ. Training of the trainers (TOT) course book. Scholars' Press: May 2021 (ISBN: 978-613-8-95332-6).
- Al-Mosawi AJ. Instruction methods course for physicians: A practical course. Scholars' Press: May 2021 (ISBN: 978-3-639-66435-5).
- Al-Mosawi AJ. Training knowledge for physicians and medical schools’ instructors.1st ed., Saarbrücken; LAP Lambert Academic Publishing: 2020 (ISBN: 978-620-2-67481-2).
- Al-Mosawi AJ. Ausbildungswissen für Ärzte und Ausbilder von medizinischen Schulen (German Edition). Verlag Unser Wissen: 2020 (ISBN-10: 6202628405, ISBN-13: 978-6202628402).
- Al-Mosawi AJ. Formação de conhecimentos para médicos e instrutores das escolas médicas (Portuguese Edition) Edições Nosso Conhecimento: 2020 (ISBN-10: 6202628464, ISBN-13: 978-6202628464).
- Al-Mosawi AJ. Wiedza szkoleniowa dla lekarzy i instruktorów szkół medycznych (Polish Edition). Wydawnictwo Nasza Wiedza: July 2020 (ISBN-10: 6202628456, ISBN-13: 978-6202628457).
- Al-Mosawi AJ. Instruction methods: An introductory course for physicians. LAP Lambert Academic Publishing: Oct 2021 (ISBN-13: 978-620-4-21067-4, ISBN-10: 620421067X).
- Al-Mosawi AJ. Principles of instruction for board certified physicians: An accredited course. LAP LAMBERT Academic Publishing: December, 2021 (ISBN: 978-620-4-72764-6).
- Al-Mosawi AJ. Essentials of instruction methods for board certified physicians: An accredited course. Scholars' Press, Nov, 2021(ISBN: 978-613-8-96565-7).
- Al-Mosawi AJ. Metodi didattici: Un corso introduttivo per medici (Italian edition). Edizioni Sapienza: 2022 (ISBN-13: 978-620-4-89832-2, ISBN-10: 6204898329).
- Al-Mosawi AJ. Méthodes d’enseignement: Un cours d'introduction pour les médecins (French edition). Editions Notre Savoir: 2022(ISBN-13: 978-620-4-89831-5, ISBN-10: 6204898310).
- Al-Mosawi AJ. Métodos de instrução: Um curso introdutório para médicos (Portuguese edition). Edições Nosso Conhecimento: 2022(ISBN-13: 978-620-4-89833-9, ISBN-10: 6204898337).
- Al-Mosawi AJ. Case studies in pediatric psychiatry: An approach to deep learning. 1st ed., Saarbrücken; LAP Lambert Academic Publishing: 2020 (ISBN: 978-620-2-52071-3).
- Al-Mosawi AJ. Fallstudien in der pädiatrischen Psychiatrie: Ein Ansatz zum Deep Learning (German edition). Verlag Unser Wissen :2021(ISBN-13: 978-620-3-29423-1, ISBN-10:62032942 33).
- Al-Mosawi AJ. Case studies in pediatrische psychiatrie: Een benadering van diep leren (Dutch edition) .Uitgeverij Onze Kennis: 2021 (ISBN-13: 978-620-3-29429-3, ISBN-10:6203294292).
- Al-Mosawi AJ. Studi di casi in psichiatria pediatrica: Un approccio all'apprendimento profondo (Italian edition). Edizioni Sapienza: 2021 (ISBN-13: 978-620-3-29424-8, ISBN-10:6203294 241).
- Al-Mosawi AJ. Métodos de enseñanza: Un curso de introducción para médicos (Spanish edition). Ediciones Nuestro Conocimiento: 2022 (ISBN-13: 978-620-4-89830-8, ISBN-10: 6204898302).
- Al-Mosawi AJ. Opleidingskennis voor artsen en instructeurs van medische scholen (Dutch Edition). Uitgeverij Onze Kennis: July 14, 2020 ISBN-10: 6202628448 , ISBN-13: 978-6202628440).
- Al-Mosawi AJ. Unterrichtsmethoden: Ein Einführungskurs für Mediziner (German edition). Verlag Unser Wissen:2022 (ISBN-13:978-620-4-89829-2,ISBN-10:62048982 99).
- Al-Mosawi AJ. Formazione dei medici e degli istruttori delle scuole di medicina (Italian edition). Edizioni Sapienza : 2020 (ISBN-13:978-620-2-62843-3, ISBN-10:620 262843X).
- Al-Mosawi AJ. Методы обучения: Вводный курс для врачей (Russian edition). Sciencia Scripts : 2022 (ISBN-13: 978-620-4-89834-6, ISBN-10: 6204898345).
- Al-Mosawi AJ. Conocimientos de capacitación para médicos e instructores de escuelas de medicina (Spanish edition). Ediciones Nuestro Conocimiento: 2020 (ISBN-13:978-620-2-62841-9, ISBN-10:620262 8413).
- Al-Mosawi AJ. Formation des connaissances des médecins et des instructeurs des écoles de medicine (French edition). Editions Notre Savoir: 2020 (ISBN-13:978-620-2-62842-6, ISBN-10:6202628421).
- Al-Mosawi AJ. Обучающие знания для врачей и инструкторов медицинских вузов (Russian edition). Sciencia Scripts: 2020 (ISBN-13: 978-620-2-62847-1, ISBN-10: 6202628472).


