Archive : Article / Volume 2, Issue 1
Case Report | DOI: https://doi.org/10.58489/2836-5070/005
Obesity: a clinicianâs perspective
Correspondng Author: Hector M Baillie
Citation: Hector M Baillie, (2023). Obesity: a clinicianâs perspective. Journal of Obesity and Fitness Management.2(1). DOI: 10.58489/2836-5070/005.
Copyright: © 2023, Hector M Baillie, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received Date: 2023-01-10, Received Date: 2023-01-10, Published Date: 2023-01-21
Abstract Keywords:
Abstract
Introduction
I am sometimes referred to as a medicine/geriatric specialist, but I credit geriatricians with a lot more smarts with the elderly (osteoporosis, cognitive decline, movement limitations, social interaction) than I do. But I might call myself an internal medicine/metabolic syndrome doctor, given the size and shape of my referral population.
In Roman times, it was a sign of success and wealth to be overweight. I remember seeing a statue on top of a sarcophagus (of the occupant), who in life was clearly obese. It was also a defence against disease and famine, which were unpredictable in occurrence and life-threatening in severity. Intermittent war, blight, and social upheaval made the lot of our ancestors quite grim.

I don’t think I have to go far to find a patient example. Janice Munro is 53, short (5feet 2in) and heavy (“over 320lb”). I have been asked to see her because of intractable hypertension, a condition that didn’t run in her family. She avoids salt and anti-inflammatories, isn’t diabetic (sugars are “high normal, A1c 6.4”) and walks to the shops every day with her toy poodle, Max. She wonders why her 3 anti-hypertensive drugs aren’t working (HCTZ 25mg od, Amlodipine 5mg bid, Ramipril 10mg od). She’s averaging 165/90 on her home monitor. “I think I must have a slow metabolism, or a hormone imbalance”.
We spend some time going over the rationale for treatment (stroke prevention, reduction in cardio-renal failure and arrhythmia, etc.) - just so we are on the same page. She seems motivated, and drug compliant. But she has never been keen on lifestyle changes. She’d rather take another pill than lose weight. Maybe it is just what she was used to all her life: high carb snacks, a certain comfort level with oversize garments, avoidance of high-impact activity.
I also review her sleep pattern. She snores, has daytime somnolence, and terrible reflux, so she knows I am going to discuss sleep apnoea.
Nothing comes out of her history and physical: I make a note I have not looked in her fundi, nor done a neurologic exam. But heart sounds seem normal, and she doesn’t look Cushingoid. No bruits to comment upon, and her pulse is regular 75bpm. Her blood pressure was 165/90.
Her bloodwork, including TSH, was normal (although she has a climbing blood sugar). Her EKG shows sinus rhythm and voltage criteria for hypertension. Does this description sound familiar? You know she’ll be back in a few years with a GFR 50, FBS 7.5 and paroxysmal atrial fibrillation. This is bread and butter stuff.
Interesting to note is that she was laid off from her part-time receptionist job last year. Her income and her good food options are now quite limited. She admits she cuts back on amlodipine when her ankles swell, and she occasionally forgets her ACEi drug. She doesn’t know her sister’s medical history, but thinks she had trouble with her kidneys before dying at age 48. She treats her migraines with Advil, but knows they aren’t good for blood pressure and reflux. She is anxious about her son (on probation). She doesn’t want to discuss her alcohol issues. “Don’t worry, I’ve given up before - lots of times,” she says. Hmmm.
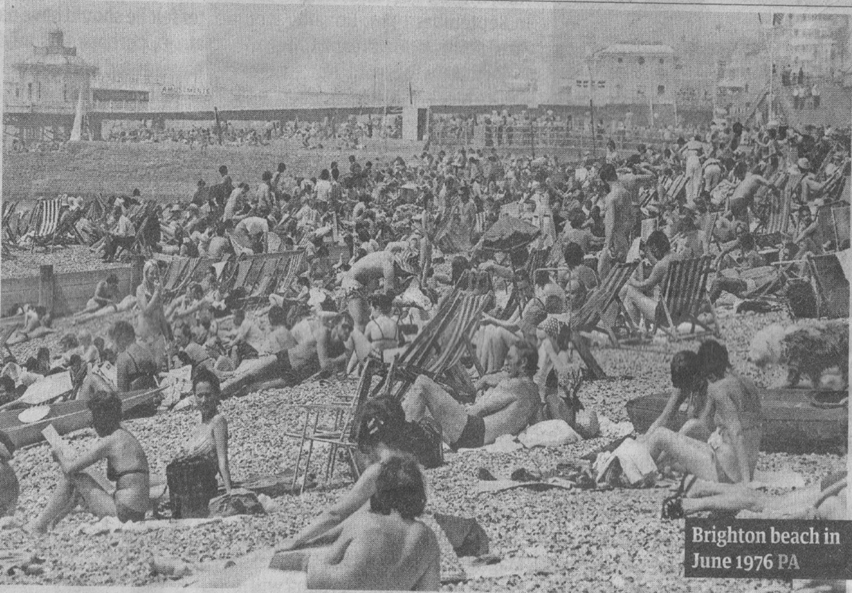
I came across a photo in the UK paper, The Guardian, from 1976. (1) It was taken on Brighton Beach. A large number of sunbathers, all looking slim and relatively healthy. Their average daily caloric intake was 2,280 calories. Nowadays, that number is 2,400-3,200. You can bet your bottom dollar that Brighton Beach is now populated by overweight people. 3% of Brits were obese then, 25% now. Why? Less physical activity (people drive to work, or work from home); diets are much more carbohydrate-rich (it’s in lots of our processed food); and there hasn’t been a recent famine in North America or the UK. Stress does play a part too - we have COVID pandemic, a war in Ukraine, financial-social-and-political disparities, and high expectations of our healthcare system - and stress eating is calorie rich.
I told Janice what I told my wife 2 years ago.
“You have to stop washing my suit, it’s shrinking! I can’t button up my trousers.”
Sheena stopped, turned, looked me in the eye and said:
“I don’t wash your suits. You are fat and ugly, do something about it!”
I explained to her that I have a balanced diet - bread, pasta, pizza, rice, potatoes, beer, wine and candy.
“Balanced on the edge of the abyss,” she replied. I find out I am a sugar-junkie, and explore exotic options, like salads, nuts, cheese, diet-pop and fruit.
After 2 months of ‘re-programming’, I lose 20lbs in weight and my trousers now fit. I get odd looks, like I have cancer or something.
“I’m on a diet,” I explain. I still get odd looks.
I was never athletic, so my 3-times-a-day dog walk has to suffice (I tell myself Cassie couldn’t handle more, and realize this is an obvious lie).
So, Janice and I part friends. She is more-educated, and maybe more-motivated. We need to get on top of her carb issue - likely from 1/2 bottle of ‘red’ wine a day, and her liberal intake of bakery products. I tell her ankle swelling is cosmetic at this point (amlodipine relaxes peripheral capillaries, leading to tissue edema), and that support hose, periodic leg elevation and weight loss might deliver results. Her normal BNP is noted.
I know that I if lose her confidence, her adherence to even simple advice will vanish. Over time, she becomes her own best life-coach. She changes her diet, reduces her alcohol intake, and becomes a poster-girl for CPAP therapy. Her blood pressures now average 139/80, and her cardiovascular risk is much improved. We can work on sugar, lipids, weight and stress another day. A work in progress, really.
References
- Monblot, G We’re not eating more… The Guardian 24Aug2018 p48


