Article In Press : Article / Volume 3, Issue 2
- CLINICAL IMAGES | DOI:
- https://doi.org/10.58489/2836-5127/022
Multi-slice CT angiography of a ruptured MCA bifurcation berry aneurysm: Clinical images
1Radiology Specialist, Radiology Department, Al-Namas General Hospital, Ministry of Health, Al-Namas City, Saudi Arabia.
Abdulwahab F. Alahmari *
Abdulwahab F. Alahmari. (2024). Multi-slice CT angiography of a ruptured MCA bifurcation berry aneurysm: Clinical images. Radiology Research and Diagnostic Imaging. 3(1); DOI: 10.58489/2836-5127/022
© 2024 Abdulwahab F. Alahmari, this is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- Received Date: 23-05-2024
- Accepted Date: 01-06-2024
- Published Date: 06-06-2024
Multislice; Computed Tomography; Aneurysm; Congenital.
Abstract
This is a case of a 60-year-old female patient who came to the emergency room complaining of a severe headache and a CT scan for the brain was requested. A plain CT was done to rule out any pathology. The plain CT shows a right temporal intra-parenchymal acute hematoma with surrounding vasogenic edema see (Figs. 1 and 2). The pre-contrast reveals a rounded (15×13 mm) area of intermediate attenuation (isodense to grey matter) at the anterior margin of the hematoma, which indicates the possibility of an aneurysm. An angiographic study of the brain was done to evaluate the MCA. A 100 cc of non-ionic contrast media was injected via a superficial upper limb venous cannula, followed by a spiral acquisition in the arterial phase from the upper chest up to the brain. The post-contrast reveals a berry aneurysm arising from the right MCA bifurcation as a saccular aneurysmal dilatation see (Figs. 3 to 6). Also, the CT shows the patent average calipers of ICA and ECA on both sides. There is no evidence of arterial stenosis, occlusion, or AV malfunction. Also, normal vertebral arteries were seen on the brain angiography scan. The patient received a referral to a tertiary hospital, where she underwent a surgery in the interventional radiology unit and was confirmed to have a congenital aneurysm. It is important to differentiate bifurcation from trifurcation aneurysms. The prevalence of MCA bifurcation aneurysms is 18–36% of all intracranial aneurysms and it affects women more than men [1]. Berry aneurysms usually mimic a hemorrhage [2].
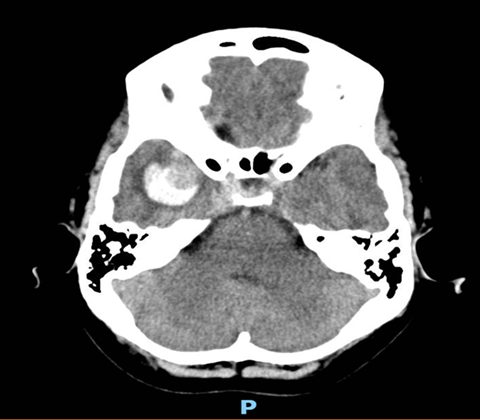
Fig 1: An axial plain brain CT scan reveals a right temporal lobe hematoma.
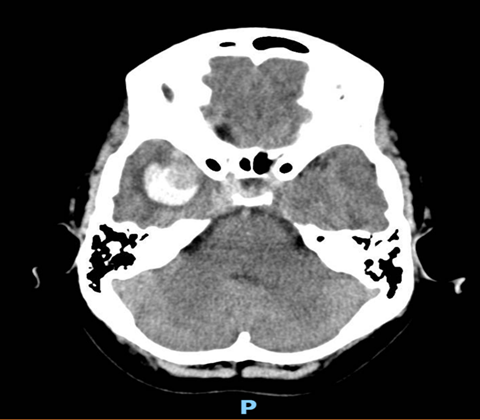
Fig 2: An axial plain brain CT scan reveals a right temporal lobe hematoma.
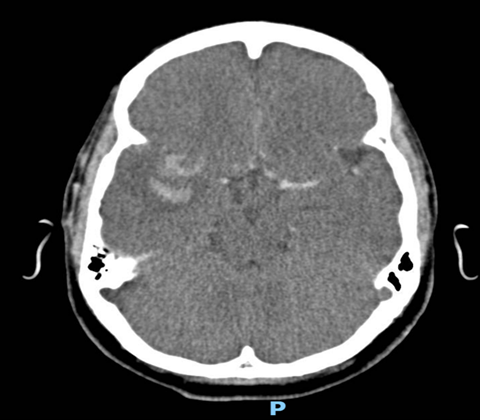
Fig 3: An axial post-contrast brain CT scan reveals a dilated right MCA and filled aneurysm with a hypodense part, which confirms the berry aneurysm diagnosis.
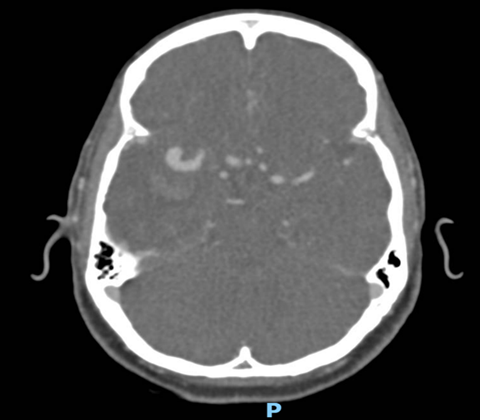
Fig 4: An axial post-contrast brain CT scan reveals a dilated right MCA and it shows that the aneurysm starts from the bifurcation of the MCA.

Fig 5: A coronal post-contrast brain CT scan reveals a dilated MCA and filled aneurysm.

Fig 6:A sagittal post-contrast brain CT scan reveals a dilated MCA and filled aneurysm. The aneurysm appears to be arising from the bifurcation of the MCA.
References
- Wang, S., Li, L., Gao, H., Zhang, K., Shao, Q. J., Li, T., & Gao, B. (2023). Middle cerebral artery bifurcation aneurysms are associated with patient age, sex, bifurcation angle, and vascular diameters. Scientific Reports, 13(1), 22844.
- Alahmari A. 3D TOF MRA of Thrombosed Berry Aneurysm Mimic Pontine Hemorrhage. Clin Res Neurol 2022;4(1):11-16. DOI: 10.33309/2638-7662.04010


